Keywords: Spear flap; nasolabial turnover flap; nasal ala reconstruction; basal cell carcinoma; case series
Authors: Lukas Kure-Rosenberg, Matilda Svenning, Mille Vissing, Magnus Balslev Avnstorp. Dept of Plastic & Breast Surgery, Roskilde, Zealand University Hospital, Denmark.
Abstract
Background: Reconstructing the full thickness of the nasal ala is technically challenging because it requires restoring contour, lining, and airway patency all at once. The Spear flap, also known as the nasolabial turnover flap, remains a useful single-stage option for selected lateral alar defects. Cases: Two elderly women presented with recurrent basal cell carcinoma of the ala nasi following multiple prior curettages. In case 1, excision resulted in a 20 × 12 mm through-and-through alar defect. In case 2, a recurrent lesion on the left alar measuring 11 × 8 mm initially required staged margin control before final reconstruction. Technique: Both defects were reconstructed using a cheek-based Spear flap after frozen-section-guided excision. Flap design was customized to recreate internal lining and external coverage while minimizing distortion of the alar rim and vestibule. Results: Both flaps remained viable, with no evidence of ischemia or venous congestion. Case 1 achieved complete oncologic clearance and healed with a stable contour; mild residual vestibular fullness did not warrant revision. In case 2, staged clearance allowed for delayed single stage inset, and early healing proceeded without complications. Conclusion: For recurrent through-and-through alar defects, the Spear flap is a reliable and practical reconstructive option. Especially in elderly patients with comorbidities or competing health issues, it provides dependable vascularity, good tissue match, and restores the alar subunit without the complexity of multi-stage procedures.
Patient medical history
Case 1 (left image) A 90-year-old woman was referred for recurrent basal cell carcinoma of the ala nasi after multiple previous curettages performed in a private dermatology practice in october 2025. Preoperative biopsy inhouse demonstrated an infiltrative subtype. Her medical history included hypertension and ischemic heart disease. She had no smoking history and reported drinking 21 units of alcohol per week. Case 2 (right image) A 79-year-old woman presented with recurrent basal cell carcinoma of the left ala nasi after multiple previous curettages. Histology revealed nodular and infiltrative components, and an in-house 2 × 2 mm punch biopsy confirmed infiltrative basal cell carcinoma. Her medical history was significant for carcinoma of the cardia, and she was undergoing immunotherapy. She had no smoking history and did not report alcohol use.


Before and After
Patient examination
Case 1
Tumor excision in October 2025, resulting in a 20 × 12 mm through-and-through alar defect. Frozen section analysis indicated clear margins except at the 12 o’clock margin, where residual tumor was within 5 mm; thus, an additional 4 mm rim was re-excised at that site. Final histopathology confirmed complete excision.
Case 2
The clinical lesion initially measured 11 × 8 mm. During the first operation, frozen section analysis showed residual tumor at the 6 o’clock margin and the deep margin. Re-excision resulted in a through-and-through defect, and definitive reconstruction was deferred while the defect remained open pending margin control.
Pre-operative considerations
Reconstruction of the nasal ala is one of the more challenging tasks in facial reconstruction because even minor tissue loss can affect a prominent free margin and compromise the external nasal valve. Successful repair must restore the contour, preserve the alar-facial sulcus, and provide sufficient internal lining while ensuring good scar concealment. The nasal subunit concept remains especially relevant in this area, where scar placement and maintaining convexity greatly influence the aesthetic outcome. [1].
For selected full-thickness lateral alar defects, the nasolabial turnover flap described by Spear provides a single-stage option using adjacent cheek tissue with a good color and texture match [2,3]. Modern reconstructive algorithms still focus on tailored choices based on defect depth, size, and subunit involvement, with local flaps remaining essential when graft-only reconstruction cannot adequately restore contour or lining. [4].
We present two elderly patients with recurrent basal cell carcinoma of the ala nasi treated with oncologic excision and Spear flap reconstruction. Both cases demonstrate the importance of a single-stage local approach for recurrent disease, especially when prior destructive treatments and patient-specific factors limit reconstructive options.
Case 1: Preoperative markings
Preoperative view of recurrent alar basal cell carcinoma after multiple prior curettages with planned Spear flap markings in the cheek/nasolabial reservoir.
Case 1: Excision of tumor
Tumor was excised including all layers of the right lateral alar. Tumor can be seen in the lateral interior mucosa of the nose and the interior marking (left picture) demonstrate where excision was planned to from tumor side (5mm). Complet sample for histopatological examination and lastly, through-and-through defect after excision and margin re-excision. The tumor excision, resulting in a 20 × 12 mm complete alar defect involving the central bulbous part of the nose. Frozen section analysis indicated clear margins except at the 12 o’clock margin, where residual tumor was within 5 mm; thus, an additional 4 mm rim was re-excised before reconstruction.
Case 1: Flap elevation
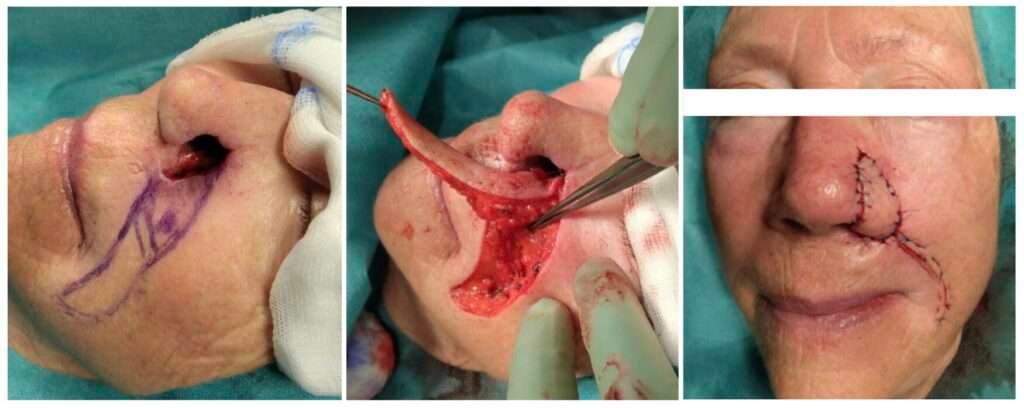
The defect was reconstructed in the same session using a Spear flap. A cheek-based flap was designed along the nasolabial fold, raised while preserving subcutaneous vascularity, turned medially to recreate the internal lining, and folded outward to cover the external alar rim. The flap was carefully raised with respect to the underlying perfusion vessels pointed out (left image). Complete elevation of the flap with demonstration of the turnover design (central). The flap is anchored inside-out with suturing of the nasal lining, subcutaneous plan, and finally the exterior skin (right). The flap was inset without undue tension.
Case 1: Immediate postoperative
The immediate postoperative appearance with final reconstruction appeared viable with no signs of ischemia or venous congestion. At suture removal (not shown), the reconstruction continued to appear viable with no defects or sings of infection.

3mo Follow-up
During later follow-up, the contour remained stable. Mild vestibular fullness persisted, but the patient opted not to pursue secondary thinning or revision
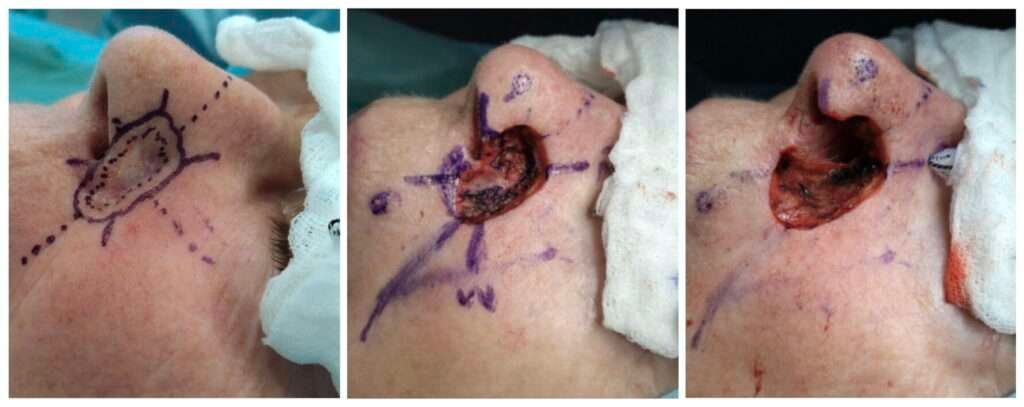
Case 2: Excision of tumor
The clinical lesion initially measured 11 × 8 mm (left). During the first surgery, frozen section analysis showed residual tumor at the 6 o’clock margin and the deep margin (central). Re-excision resulted in a through-and-through defect involving a larger portion of the mucosa (right), and definitive reconstruction was deferred while the defect remained open pending expedited histopatological margin control.
Case 2: Flap elevation
At the second surgery nov. In 2025, frozen sections from the remaining superior margin (10 to 2 o’clock) were clear and verified previous histology, allowing for definitive reconstruction. A Spear flap was designed from the adjacent cheek and transposed in a turnover fashion to recreate the alar lining and outer cover in a single stage. The flap perfused well during surgery.
Pearls
u0026#8226; Secure oncologic control before definitive inset, particularly in recurrent infiltrative disease [1,4].
u0026#8226; Design the flap from supple cheek/nasolabial tissue with sufficient length to recreate both internal lining and external cover [2,3].
u0026#8226; Preserve the alar-facial sulcus and place scars along natural subunit boundaries whenever feasible [1].
u0026#8226; Prioritize a tension-free inset and preserve flap bulk initially; secondary refinement is safer than aggressive primary thinning [3,5].
Pitfalls
u0026#8226; Proceeding to definitive reconstruction before margin control is complete in recurrent disease can jeopardize both oncologic safety and flap planning.
u0026#8226; A broad or tensioned proximal pedicle may produce commissure traction, vestibular narrowing, or alar malposition [3,5].
u0026#8226; Direct closure or graft-only reconstruction of a through-and-through alar defect may flatten the ala and fail to restore lining or free-margin support adequately [4].
u0026#8226; Over-thinning the flap during the index procedure may compromise vascularity and should be avoided when postoperative bulk can be observed and revised later if needed.
Post-operative plan
Case 1:
At suture removal, the reconstruction appeared viable with no signs of ischemia or venous congestion. During later follow-up, the contour remained stable. Mild vestibular fullness persisted, but the patient opted not to pursue secondary thinning or revision
Case 2:
The patient was seen 10 days postoperatively for suture removal, and healing was uncomplicated. No further routine follow-up was scheduled because of other ongoing oncologic treatment so patient wished no further corrections
Conclusion:
The Spear flap remains a reliable single-stage option for specific recurrent through-and-through defects of the nasal ala. In elderly patients and in cases where previous treatments or other disease burdens make complex staged reconstruction less desirable, it provides dependable vascularity, a good tissue match, and restoration of the alar subunit with satisfactory functional and aesthetic results.
References
Burget GC, Menick FJ. The subunit principle in nasal reconstruction. Plast Reconstr Surg. 1985;76(2):239-247. doi:10.1097/00006534-198508000-00010.
Spear SL, Kroll SS, Romm S. A new twist to the nasolabial flap for reconstruction of lateral alar defects. Plast Reconstr Surg. 1987;79(6):915-920. doi:10.1097/00006534-198706000-00010.
Kroll SS. Nasal alar reconstruction using the nasolabial turnover flap. Laryngoscope. 1991;101(10):1127-1131. doi:10.1288/00005537-199110000-00016.
Chen C, Patel R, Chi J. Comprehensive algorithm for nasal ala reconstruction: utility of the auricular composite graft. Surg J (N Y). 2018;4(2):e55-e61. doi:10.1055/s-0038-1639581.
El Habr C, Vinelli G, Tinklepaugh A, Ciocon D. Reconstruction of an alar defect with a fusiform nasolabial turnover flap with a proximal, superiorly tapered apex. J Craniofac Surg. 2018;29(1):e20-e21. doi:10.1097/SCS.0000000000003990.