Keywords: Eyelid reconstruction, Hughes flap, tarsoconjunctival flap, periosteal flap, periorbital, scc, cheek rotational flap, Z-plasty
Authors: Sondre F. Koren (MD) and Jette B. Løvenwald (MD). Roskilde, Zealand University Hospital, Denmark.
Abstract
An 83-year-old male with atrial fibrillation, stage 4 chronic kidney disease, chronic heart failure, monoclonal gammopathy of undetermined significance (MGUS), and glaucoma presented with a 35 × 35 × 15 mm ulcerated squamous cell carcinoma (SCC) of the lateral right lower eyelid. Frozen section-guided full-thickness excision was performed under general anaesthesia. Reconstruction was accomplished in two stages. In the first stage, a combined pedicled tarsoconjunctival flap and a laterally-based periosteal flap (posterior lamella), and a cheek rotation flap (anterior lamella) were used. Frost sutures provided corneal protection during the 4-week inter-stage interval. In the second stage, flap division was performed under general anaesthesia, incorporating Müller’s muscle release to prevent upper eyelid retraction. A small dehiscence at the medial flap junction had resulted in a minor notch, which was ultimately resolved with Z-plasty and release of the underlying inferior scar contracture on the cheek. Final histopathology confirmed highly differentiated SCC with clear margins. The multidisciplinary tumour board found no indication for adjuvant therapy. At 23 days following flap division, the patient was satisfied with the functional and aesthetic result.
Patient medical history
The patient underwent surgery after a 7-week history of a growing tumour of the cheek and lateral lower eyelid. The punch biopsy reported keratoacanthoma/highly differentiated SCC. The tumour had been observed to assess for spontaneous regression, but continued to grow. He had stage 4 chronic kidney disease, treated with Darbepoetin alfa (Aranesp), and glaucoma treated with Latanoprost eye drops, which he had not been taking for several months, with no documented decline in vision. His atrial fibrillation was managed with warfarin (Marevan) and beta-blockers. He was a non-smoker, ambulatory without assistive devices, living independently, and managing activities of daily living without assistance.


Before and After
Patient examination
The patient presented with a 35 × 35 × 15 mm sharply demarcated, ulcerating tumour situated on the right lateral lower eyelid and zygomatic region, not involving the mucocutaneous junction, and causing a mild mechanical ectropion. The tumour was mobile over the underlying rigid structures. No regional lymph nodes were palpable.
Pre-operative considerations
Due to the localisation of the tumour and its sharp clinical demarcation, a decision was made – following consultation with a senior colleague – to excise the tumour with a 5 mm margin. This meant that approximately half of the eyelid would be removed by full-thickness excision, and given the tumour’s thickness, invasion of the orbicularis muscle was suspected. This warranted reconstruction of the posterior lamella with a tarsoconjunctival flap and a periosteal flap, and of the anterior lamella with a cheek rotation flap.
The patient’s warfarin (Marevan) was paused in accordance with regional guidelines, and prophylactic antibiotics were planned at a reduced dose due to the patient’s chronic kidney disease. Given the anticipated duration of the procedure and the discomfort associated with operating in this region, the operation was performed under general anaesthesia.
Given the patient’s glaucoma, his ophthalmologist was consulted regarding the safety of pausing Latanoprost eye drops during the inter-stage period, as the operated eyelid would remain closed until flap division.
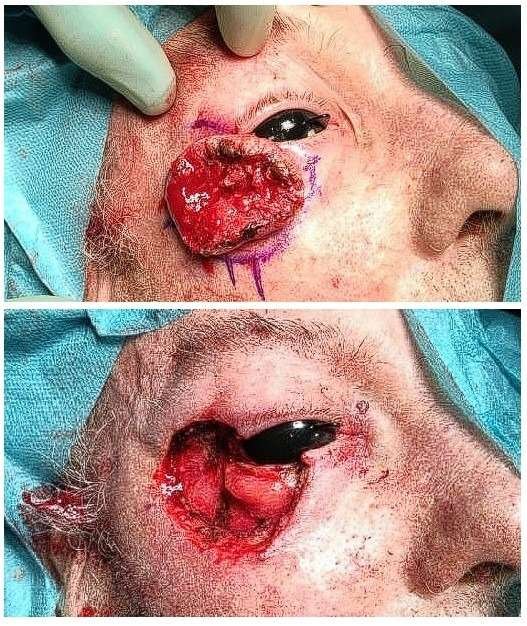
Excision of the tumor
The tumour was marked with a 5 mm margin, and a protective shell was placed on the cornea. The excision was taken down to the preseptal fat. Frozen sections were sent, and all margins returned negative. The upper lateral canthal ligament was left intact; the lower was excised.
Raising the tarsoconjunctival flap as the first part of reconstructing the posterior lamella
A stay suture was placed through the grey line of the upper eyelid, and a Desmarres retractor was placed, facilitating retraction of the lid and keeping it everted during the procedure. A tarsoconjunctival flap from the upper eyelid was marked, preserving 4 mm of tarsus inferior to the flap to maintain the upper eyelid framework. As the tarsal plate tapers towards the lateral edges, the flap was harvested more medially than the defect to achieve the required length, while preserving the aforementioned 4 mm of tarsus. The levator tandon was divided from the tarsal plate, along with a portion of Müller’s muscle, leaving a pedicle of the remaining muscle and the conjunctiva. The flap was advanced inferiorly to the defect and sutured tension-free with 5-0 and 6-0 Vicryl.

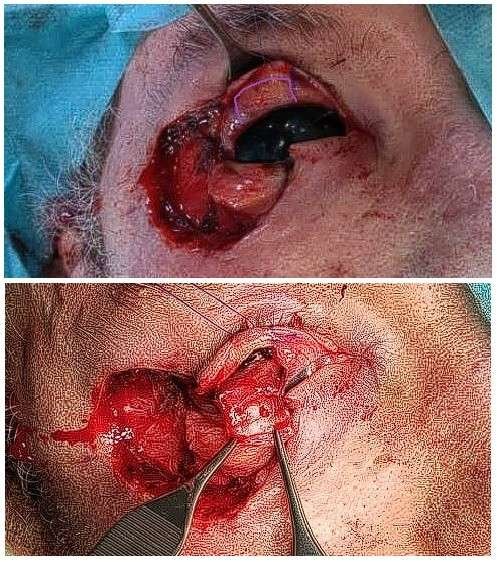
Periosteal flap for the second part of reconstructing the posterior lamella
A periosteal flap was designed with a 30-degree superior angulation relative to the intercanthal horizontal line, to maintain a superior vector and protect against ectropion. The flap was raised with the distal portion incorporating temporal fascia, harvested slightly longer than required and with a width of 7–8 mm. After turning it over as a hinge flap, the length was trimmed to achieve appropriate tension for suspension of the lower posterior lamella, and the flap was sutured to the tarsoconjunctival flap with 5-0 PDS mattress sutures. The upper lateral canthal ligament was then sutured to the periosteal flap to reconstruct the common canthal ligament and recreate the sharp angle between the upper and lower canthal ligaments, using 5-0 Prolene.

Reconstructing the anterior lamella
The anterior lamella was reconstructed with a classic cheek rotation flap raised on the SMAS. A pexy of the flap to the periosteum of the lateral orbital rim was performed with 3-0 PDS. The flap was then closed with 4-0, 5-0, and 6-0 Vicryl and 5-0 and 6-0 Prolene over a glove drain, which exited anterior to the ear.

Postoperative photo after completion of the first stage of the reconstruction
After the photograph was taken, Frost sutures were passed through the grey line and taped to the forehead to protect the cornea and relieve tension on the reconstruction.

Dividing the flap
Pearls
When planning the reconstruction, divide it into the posterior and anterior lamella. This breaks a complex reconstruction into more manageable parts.
Place stay sutures through the grey line of the upper eyelid. This, in combination with a Desmarres retractor, greatly facilitates the assistant’s ability to maintain traction on the eyelid during surgery.
Angle the periosteal flap superiorly to reduce the risk of ectropion.
Pitfalls
Exercise caution when harvesting the temporal fascia to minimise the risk of injury to the frontal branch of the facial nerve.
Post-operative plan
Following the first stage, the importance of not discharging the patient to his home alone was emphasised, as he was now monocular due to the bridging tarsoconjunctival flap, had pre-existing glaucoma, and was on anticoagulation therapy — all of which posed a significant risk of falls and trauma. He was therefore kept admitted until a place became available at a rehabilitation facility. Sutures were removed at 7 days, on the day of discharge, and prophylactic antibiotics were continued until the same day. A standard postoperative regimen was ordered for the first few days, including head of bed elevation and a soft diet.
Following the second stage, the patient was discharged on the same day and sutures were removed at nine days. Chloramphenicol ointment was applied as topical prophylaxis during this period.
A head and neck ultrasound performed six weeks postoperatively demonstrated no evidence of lymph node metastasis.
References
Development and validation of a decision algorithm for eyelid reconstruction following oncological resection. Miotti G, Quaglia D, Novati FC, et al. World J Transplant. 2025 Jun 18;15(2):97571. doi: 10.5500/wjt.v15.i2.97571
Modified Hughes procedure for reconstruction of large full-thickness lower eyelid defects following tumor resection. Hishmi AM, Koch KR, Thomasen H, et al. European Journal of Medical Research. doi: 10.1186/s40001-016-0221-1
Hughes Procedure. EyeWiki — American Academy of Ophthalmology
Optimizing the periosteal flap for lateral eyelid reconstruction. McClellan WT, McCord C, Neusch R. Plastic and Reconstructive Surgery, 126(4):121–122, October 2010. doi:10.1097/01.prs.0000388845.97434.2e
The suspension (Frost) suture: experience and applications. Connolly KL, Albertini JG, Miller CJ, Ozog DM. Dermatologic Surgery, 41(3):406–410, March 2015. doi:10.1097/DSS.0000000000000313