Keywords: Breast cancer, Areola reconstruction, Full-Thickness Skin Graft.
Authors: Ajla Sabitovic (MD), Nanja Gotland Sundstrup (MD)
Abstract
This case describes the use of full-thickness skin graft for reconstruction of areola in a 64-year-old woman following right-sided mastectomy and delayed breast reconstruction with a DIEP flap. The patient preferred autologous reconstruction and declined tattooing or additional donor-site scars. Due to the light pigmentation on the contralateral areola, it was decided to shave the skin off as a full-thickness in the affected area, and let the following scaring in the area lead to a little change in pigmentation and contration. This approach avoided additional scarring while achieving an acceptable aesthetic result.
Patient medical history
A 64-year-old woman with a history of right-sided breast cancer underwent mastectomy in November 2022. In August 2024, the patient received a breast reconstruction with a free DIEP flap and a contralateral breast reduction. Nipple reconstruction using af full-thickness skin graft was subsequently performed in March 2025. In October 2025, the patient underwent areola reconstruction with a full-thickness skin graft on the reconstructed breast, combining the donor and recipient site around the nipple.


Before and After
Patient examination
Clinical examination revealed aesthetically pleasing results following the DIEP flap and papil reconstruction as well as a light-colored contralateral areola.
Pre-operative considerations
It was considered to use a skin-graft from the groin due to its darker pigmentation, but the patient didn’t want any additional scares. Due to the light pigmentation on the contralateral areola, a local full-thickness skin graft was harvested at the recipient site. Postoperative scarring was expected to provide mild pigmentation change and contraction to improve areola definition.
Step 1
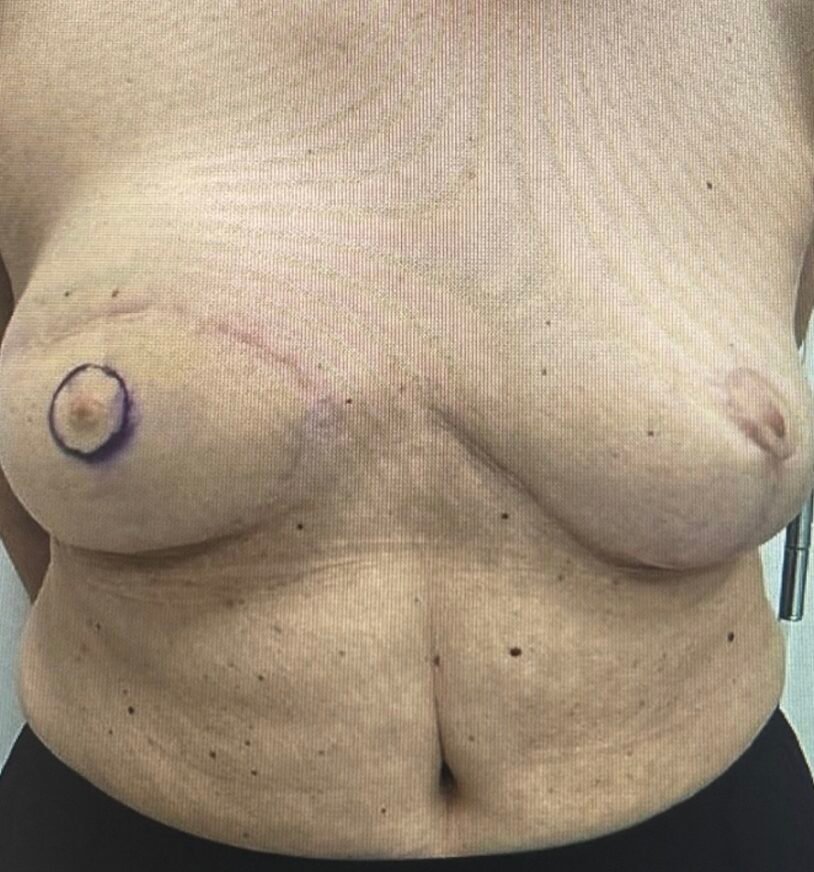
Preoperative markings performed with the patient in a standing position, showing the neoareola outlined 10 mm from the neopapilla corresponding to the size of the contralateral areola.

Step 2
Preoperative image obtained with the patient in a supine position.

Step 3
After the administration of local anesthesia (1% lidocain with adrenalin), incisions were made according to the preoperative markings around the neopapilla.

Step 4
The skin was carefully harvested as a full-thickness graft for subsequent transplantation. Hemostasis was performed.
Step 5
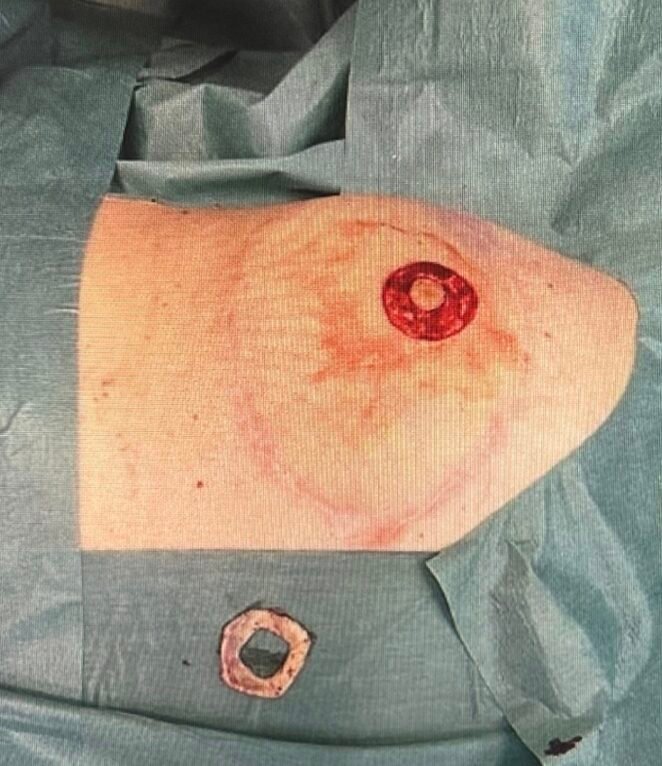
The image shows the donorsite of the full-thickness skin graft, as well as the harvested full-thickness skin graft.

Step 6
The harvested full-thickness skin graft placed on the recipient site, forming a donut-like shape around the neopapilla.

Step 7
The outer linning of the full-thickness graft was sutured with nylon 5-0.

Step 8
The image shows the suturing of the inner linning of the full-thickness graft around the neopapilla with nylon 5-0 and the final postoperative result.

Step 9
The result 10 days postoperative.

Step 10
The postoperative result after 3 months.
Pearls
1. Three-dimensional reconstruction potential.
2. Durability.
3. This technique is straight forward and well-suited for outpatient or clinical settings.
4. No additional scars are created.
5. Donor site morbidity is minimal.
Pitfalls
1. Surgical procedure compared with tattooing.
2. Donor/recipient site morbidity
Post-operative plan
The patient was advised to maintain restricted activity regimen until suture removal 10 days postoperatively. A three month follow-up was scheduled.
References
Wolber et al. Nipple areola complex reconstruction with full thicknessskin graft and subcutaneous pedicled island flap. Ann Chir Plast Esthet 2009;54(4):365-9