Keywords: Distal radius fracture, closed reduction, fracture management, Colles’ fracture, orthopedic injury
Authors: Maria Lerche Mortensen and Philip Månsson. Institution: Department of Orthopedic Surgery, SUH Nykøbing Falster, Denmark
Abstract
A 62-year-old female presented to the emergency department after a fall from standing position, attempting to break the fall with her left hand. She presented with pain, swelling, and a visible deformity of the wrist. A distal radius fracture of Colles’ type was diagnosed. She was treated in the emergency department in accordance with local guidelines, with closed reduction using both Chinese finger traps and manual reduction with a hematoma block for analgesia. Finally, a dorsal below-elbow cast was applied, and the patient was referred for follow-up after 10-12 days.
Patient medical history
This patient was active and employed, able to take care of herself, her family and household. She had no past fractures, no relevant medication, and no known allergies.


Before and After
Patient examination
Patient history was obtained, involving circumstances of the trauma, including reasons to suspect underlying disease or other injuries. She fell while walking on a slippery surface, described the trauma as “just bad luck”, she reported no other complaints of pain, had intact memory, and had no cardiac symptoms prior to fall.
The clinical examination included inspection, palpation, and function.
Inspection: A bayonet deformity was observed, with significant swelling over the radial styloid. There were no wounds or discoloration.
Palpation: There was a palpable step-off, and pain over the distal radius. Elbow, hand and fingers were palpated without pain. Therefore, there was no suspicion of other injuries.
Function: Neurological and vascular integrity were intact. The motor function was tested: n. ulnaris – finger abduction with intact strength; n. radialis – extension of the MCP-joints; n. medianus – opposition of the first digit. The sensory function was tested: n. ulnaris – sensation of the ulnar 1 ½ digits; n. radialis – sensation of the dorsal aspect of the radial 3 ½ digits; n. medianus – sensation of the volar aspect of the radial 3 ½ digits.
The suspected diagnosis was confirmed by conventional radiographs in anteroposterior (AP) and lateral views.
Pre-operative considerations
A Colles’ fracture can be managed in different ways, depending on the patient’s age, activities of daily living, fracture morphology, and local clinical guidelines.
Treatment options include: Conservative treatment with a cast; closed reduction followed by cast immobilization; closed reduction and percutaneous Kirschner wire fixation; open reduction and internal fixation (ORIF).
In this case, the patient was active and had high functional demands for her wrist function. The fracture position was not acceptable for conservative treatment alone.
The patient was offered closed reduction in the ED, considering the general preference to minimize surgical intervention, reduce complications, and limit hospital stay. The patient was informed that the procedure might be unsuccessful, or reduction could be lost at follow-up, necessitating subsequent surgical intervention.

Radiographic assessment of dorsal angulation
Before the procedure, several features on the radiographs were assessed.
The degree of dorsal angulation was measured on the lateral view. It is defined as the angle between a line representing the long axis of the radial shaft (purple line) and a line representing the joint surface (pink line), intersecting the volar and the dorsal edges of the joint surface. The normal angulation is approximately 10 degrees volar, with minor anatomical variations. In this case, the dorsal angulation was 34 degrees dorsal, which was considered unacceptable.
Radiographic assessment of radial inclination
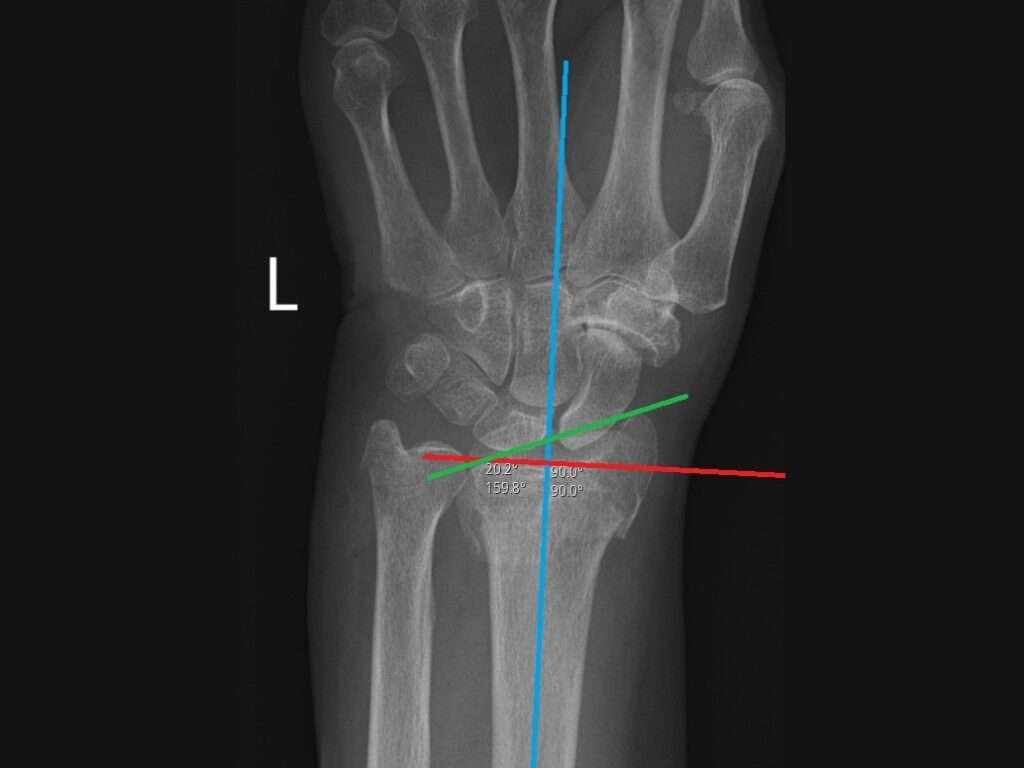
The radial inclination was measured on the AP view. It is defined as the angle between a line perpendicular to the long axis of the radial shaft (red line, (the blue line serves as a reference to guide placement of the red line)) and a line, representing the articular surface of the radius, drawn from the radial styloid to the ulnar edge of the radial articular surface (green line). This line should be placed at the central reference point of the articular surface (“the bottom of the cup”). The normal radial inclination is approximately 22 degrees. In this case, the radial inclination was 20 degrees.

Radiographic assessment of ulnar length
Ulnar variance (blue line) refers to the difference in the relative lengths of the distal articular surfaces of the ulna (yellow line) and radius (orange line). There is considerable individual variability. The ulna is often 1 mm shorter than the radius. In this case, the ulna was 3 mm longer than the radius, which was considered unacceptable.

Preparation for hematoma block
Before attempting closed reduction, a hematoma block was performed. It provides a highly effective form of analgesia prior to manipulation of the wrist.
The following materials were prepared: A drawing-up needle, injection needle, 20 ml syringe, lidocaine 1-2%, alcohol swabs, and optionally gauze. All needles were disposed in a sharps container after use.

Identifying injection site
The injection site should be slightly proximal to the fracture site. It may be easier to visualize the fracture site when comparing the clinical and radiological findings.

Preparing the injection site
The injection site is disinfected twice.

Needle insertion
The injection site should be placed slightly proximal to the fracture site. The needle is advanced until contact with the dorsal cortex is felt.

Advancing the needle to the fracture site
When the dorsal cortex is felt, the angulation is altered, so that the needle can slide along the cortex until the fracture line is reached.

Administration of local anesthetic
Blood return on aspiration indicates that the needle tip is within the fracture line. The local anesthetic should be administered there. Inform the patient that they may feel pressure and pain. Take short breaks if necessary. Continue administration until slight resistance is felt, usually after 8-12 ml. If there is a fracture of the ulnar styloid, 2-3 ml can be injected subcutaneously at that site. Wait approximately 10 minutes before manipulating the fracture.
Chinese finger traps
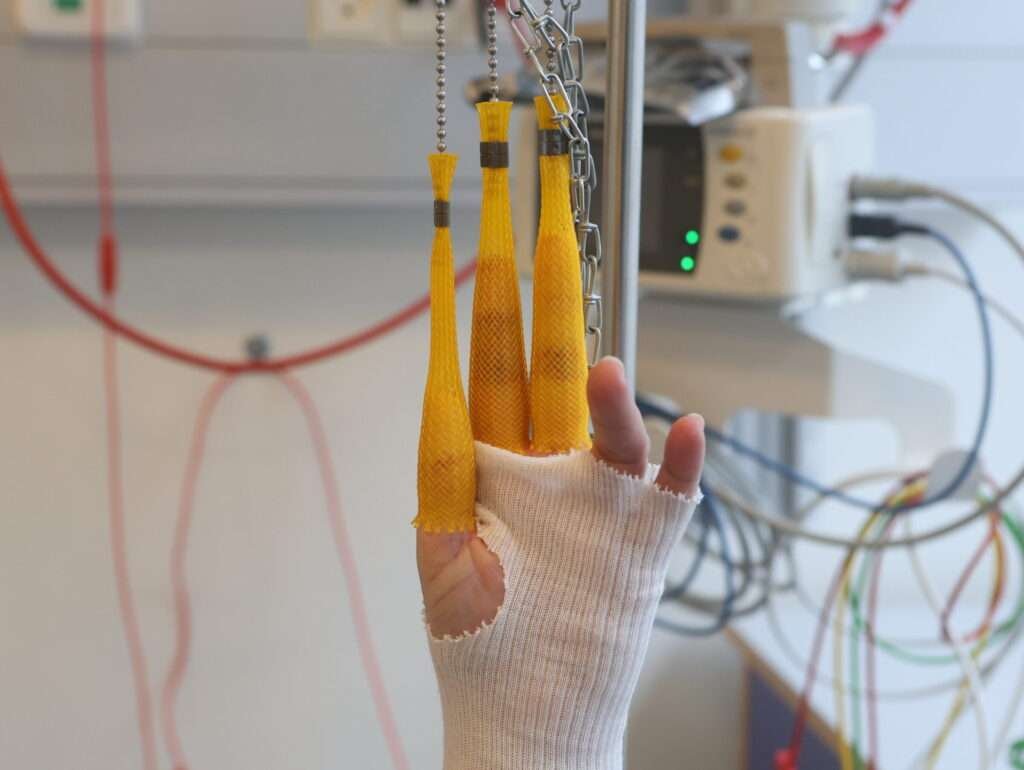
Chinese finger traps is a method that can be used alone (typically for impacted fractures and for patients with poor skin, who are at risk of wounds from manual reduction) or to induce muscle relaxation prior to manual reduction. There is no evidence that one method is superior to the other.
Ensure the hematoma block has taken effect. Select the appropriate size of fingertraps, attach them to first, second and third digits. Make sure the patient is positioned comfortably, and that there is sufficient space around the patient for manipulation and casting. The patient should lie in a supine position, with the upper arm perpendicular to the body, and the forearm perpendicular to the upper arm. The sandbag should be placed close to the elbow. Continue the traction for 20-30 minutes.

Preparation for manual reduction
Manual reduction can be performed as a standalone procedure or following finger trap traction. Ensure the hematoma block has taken effect, and that sufficient personnel are available to assist.
Have someone provide countertraction by holding a towel wrapped around the upper arm, close to the elbow, which should be flexed at approximately 90 degrees. If there are not enough personnel, the towel can be secured to a fixed object. The clinician then grasps the patient’s hand, and at least one nurse should be ready to prepare the cast.
A useful tip is to hold on to first, second and third digits if the patient has fragile skin. But otherwise just get a firm grip.

Applying dorsal pull
Begin with traction to separate the fracture ends. Then pull the hand dorsally, as if attempting to make the dorsal angulation worse; this helps release impacted segments or entrapped structures.

Applying volar pull to reestablish anatomy
Next, pull the hand volarly, to reestablish the physiological volar tilt, then maintain traction. Use the other hand to palpate the fracture site and detect a decrease in step-off.

Application of cast
If clinically satisfying, a dorsal below-elbow three-point support cast is applied while maintaining traction.

Post-casting care
Once the cast has set sufficiently and the sides can no longer be manipulated, carefully and gradually release traction and place the arm in a sling until the cast is fully dry. A new radiograph should be obtained to ensure the position.
If the post-reduction position is acceptable, the patient continues with conservative treatment. However, due to manipulation of the wrist and the unstable fracture, a follow-up clinical assessment and radiograph should be performed after 10-12 days.
Pearls
Pitfalls
Post-operative plan
In this case, closed reduction was successful. Post-reduction radiograph showed an improved position, although not perfect. The angulation was 7 degrees dorsally, the length had improved, with the ulna now at -1. The inclination remained unchanged.
The position was regarded as acceptable. The patient was discharged and was prescribed paracetamol and ibuprofen for pain management.
The patient was referred for a follow-up in 7-10 days at which time the radiographic alignment will be reassessed. If the fracture remains in position, conservative treatment is continued; otherwise, operative treatment is indicated. In conservative management, the cast is maintained for five weeks. The patient should be introduced to edema prophylaxis and finger mobilization to prevent stiffness. Some patients may require physiotherapy after cast removal. The patient can expect improvement of wrist function over the first 6 months after cast removal; some patients may continue to improve function up to a year after removal.
Due to a low-energy trauma resulting in a wrist fracture, the patient should be referred for an osteoporosis workup.
References
Closed reduction of distal radius fractures: a systematic review and meta-analysis, Hjalte Søsborg-Würtz, Sükriye Corap Gellert, Julie Ladeby Erichsen, and Bjarke Viberg. DOI: 10.1302/2058-5241.3.170063
Distal radius fractures: an evidence-based approach to assessment and management, Kalpesh R Vaghela, Diana VelazquezPimentel, Aashish K Ahluwalia, Anika Choraria, Alistair Hunter. DOI: 10.12968/hmed.2020.0006
Association Between Radiological and Patient-Reported Outcome in Adults With a Displaced Distal Radius Fracture: A Systematic Review and Meta-Analysis, Marjolein A. M. Mulders, Robin Detering, Daniel A. Rikli, Melvin P. Rosenwasser, J. Carel Goslings, Niels W. L. Schep. DOI: 10.1016/j.jhsa.2018.05.003