Keywords: Superior gluteal vessel, free flap reconstruction, lumbosacral defects
Authors: 1. Tushar Dutta, Consultant Plastic Surgeon; 2. Arun PS, Consultant Surgical Oncologist; 3. Swati Sattavan, Consultant Surgical Oncologist; Institute: State Cancer Institute, Guwahati, Assam, India
Abstract
Lumbosacral defects that are too large for local flap reconstruction should be considered for microvascular free tissue transfer. However, lack of suitable recipient vessels in the area makes the task technically difficult. Options such as thoracodorsal and inferior gluteal vessels extended with vein grafts and AV loops have been described. Each option has its own drawbacks. Despite having a short course at its origin, the superior gluteal vessel is a viable alternative. We describe here a case where the vessel was dissected out with adequate length and used as a recipient for free flap reconstruction.
Patient medical history
The patient was a 41-year-old lady with no known comorbidities. She presented to us with a large lumbosacral mass that had been growing for one year. Before visiting our center, she had been operated twice at other institutions and had recurrences after each occasion. During the last three months the mass had started to grow rapidly and caused ulceration. There was no pain or fever. There was no neurological involvement of lower limbs. Patient had an ECOG status 1.


Before and After
Patient examination
A 17x 22 cm mass was noted encompassing the left part of lumbosacral region and crossing the midline to the opposite side. The superior limit of the lesion was at the L3 vertebra and inferior extent was near the coccyx. Skin ulceration was noted at the center of the mass.
On palpation, the mass was warm to touch, hard in consistency and immobile. Skin was fixed and fixity was also noted to the underlying muscle. No tenderness was elicited.
Surrounding possible donor sites for flap harvest showed no scars.
Pre-operative considerations
Preoperative biopsy confirmed it to be a case of spindle cell sarcoma. MRI imaging showed its extension to the depth of the underlying muscles with abutment to the sacrum. Considering the multiple recurrences the patient had suffered earlier, it was decided to radically excise the tumour with wide, liberal margins. As the anticipated defect would well encroach into the opposite gluteal region, local flaps options for reconstruction were very limited. Other options such as lumbar artery perforator flaps and reverse latissimus dorsi flap were also considered, but the size and extent of the defect precluded their selection. A decision for free tissue transfer using the free latissimus dorsi flap was taken (as it could be harvested with minimal position change), with the right superior gluteal vessels as recipient. The other alternative recipient vessels such as thoracodorsal vessels and inferior gluteal vessels with vein grafts and AV loops were deemed too complex with high possibility of thrombosis.

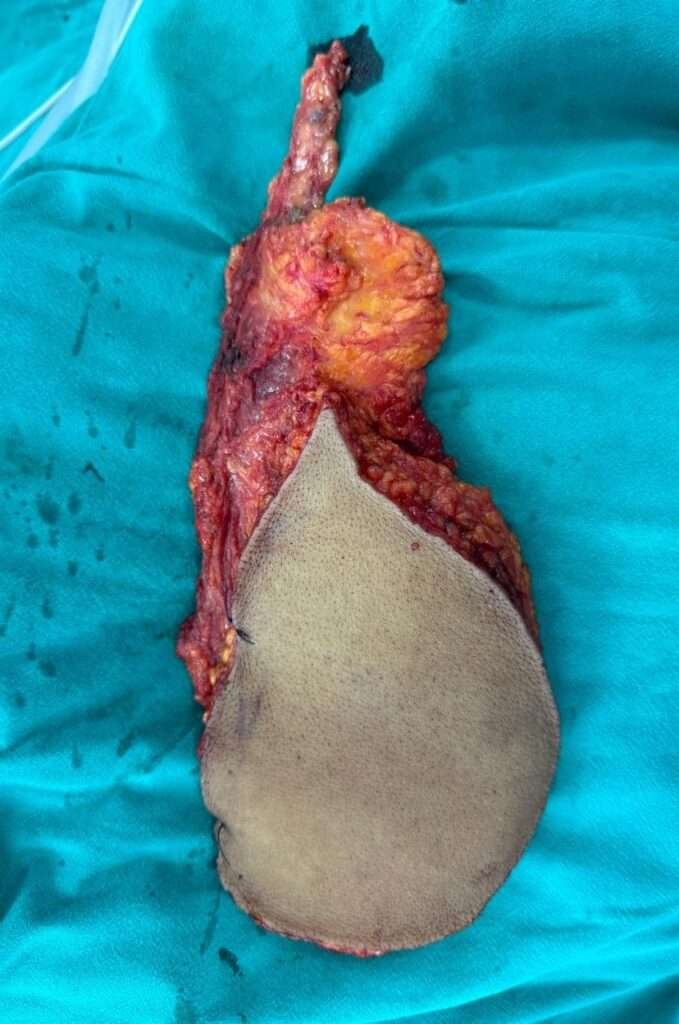
Wide local excision of the lumbosacral mass
With nearly three centimeters of margin, wide local excision of the lumbosacral mass was done with a cuff of underlying muscles. Part of the sacrum was also shaved. Frozen section biopsy was done to confirm negative margins

Post excision defect assessment
The post excision defect measured around 20 cm x 26 cm extending from the L3 vertebrae above to the coccyx below
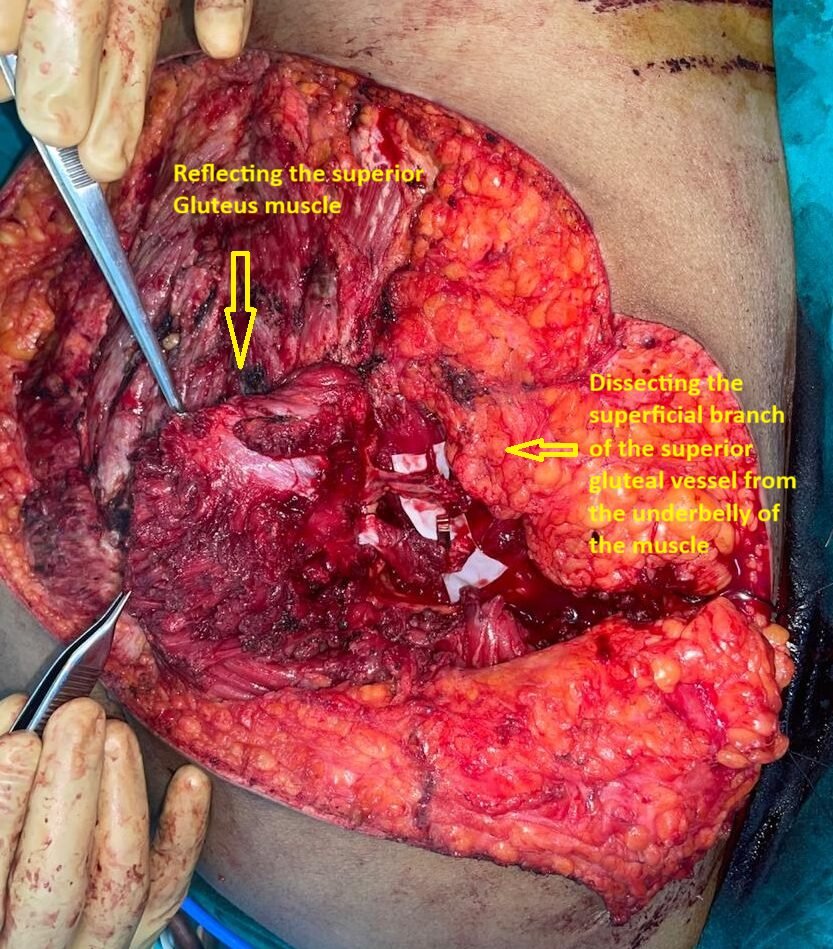
Dissection of the recipient vessel
The right superior gluteus muscle is transected at its lateral aspect (near its insertion ) and reflected medially to expose its underbelly and visualise the superficial branches of the superior gluteal vessels. The branches are then carefully dissected to gain length. The larger calibre branch is selected after confirming adequate flow. The selected branch is transposed diligently into the planned field of anastomosis. the lower part of the transected gluteal muscle is reapposed
Flap harvest
Keeping the patient slightly right lateral, a free a Myo cutaneous latissimus dorsi flap is harvested from the left side . A pedicle length of approximately 7 cm is obtained. After confirming perfusion, the flap is detached and transferred to the defect site. Part of the donor site primarily closed, rest resurfaced with Split thickness skin graft.

Micro -anastomosis
Vessel discrepancy of about 1:2 is noted between the recipient and donor vessels respectively. After dilatation and careful matching an end-to-end anastomosis of artery and vein is performed using ethilon 10-0 micro point round body sutures.

Wound Closure
After flap reperfusion, inset is completed with Latissimus dorsi muscle stretched to cover the periphery of the defect, keeping the skin paddle in the center. Part of the defect on the left side is primarily closed after placement of a corrugated rubber drain. The muscle is then skin grafted
Pearls
A bespoke design (boomerang shaped) of the skin paddle of the latissimus dorsi flap may permit primary closure of the donor site. This would avoid the need for skin grafting.
The superficial branch of the superior gluteal artery may be approached by splitting the muscle instead of transecting it. By this technique, The Superior gluteal artery perforator may be traced back to its origin. This method however is tedious, and risks injury to the vessel.
Pitfalls
After emerging at the greater sciatic notch, the superior gluteal vessel has a short length before division into superficial and deep branches. Any injury at this point may cause it to retract causing torrential bleeding that is difficult to control.
The other superior gluteal artery should be preserved, and territories of the opposite latissimus dorsi flap should not be violated. In case the free flap fails, these can be kept as lifeboats. Delay procedures may be needed to ensure reach and flap survival.
Post-operative plan
Supine or left lateral position is maintained as per the patient’s comfort. There is no need of routine anticoagulation therapy, although enoxaparin is given as per ICU protocol to prevent deep vein thrombosis. Chest physiotherapy, hydration, temperature control and pain management is essential. Flap monitoring is done by clinical evaluation and pin prick on hourly basis for the first 24 hours , followed by 2 hourly and 4 hourly during next 48 to72 hours and stopped when the patient shifted to ward. Ambulation is done after 3 days . patient is discharged after two dressing by the 10th postoperative day.
References
Park S, Koh KS. Superior gluteal vessel as recipient for free flap reconstruction of lumbosacral defect. Plastic and reconstructive surgery. 1998 Jun 1;101(7):1842-9.
Park S. Muscle-splitting approach to superior and inferior gluteal vessels: versatile source of recipient vessels for free-tissue transfer to sacral, gluteal, and ischial regions. Plastic and reconstructive surgery. 2000 Jul 1;106(1):81-6.
Hung SJ, Chen HC, Wei FC. Free flaps for reconstruction of the lower back and sacral area. Microsurgery: Official Journal of the International Microsurgical Society and the European Federation of Societies for Microsurgery. 2000;20(2):72-6.
Matschke J, Armbruster R, Reeps C, Weitz J, Dragu A. AV loop free flap: an interdisciplinary approach for perineal and sacral defect reconstruction after radical oncological exenteration and radiation in a colorectal cancer patient. World Journal of Surgical Oncology. 2019 Sep 2;17(1):154.
Özkan B, Savran S, Albayati A, Uysal ÇA. Near‐total gluteal defect reconstruction with bilateral delayed giant lumbar artery perforator flaps: A case report. Microsurgery. 2023 Sep;43(6):622-6.