Keywords: Basal cell carcinoma, scalp reconstruction, staged excision, primary closure, scalp biomechanics.
Authors: Mikkel Halborg Sørensen, MD; Nanja Gotland Sundstrup, MD; Christian Lyngsaa Lang, MD. Institution: Department of Plastic Surgery and Burns, Rigshospitalet, Copenhagen University Hos-pital, Denmark
Abstract
A 48-year-old woman was referred with a non-radically excised nodular basal cell carcinoma of the anterior scalp complicated by wound infection and dehiscence. Re-excision with 3 mm margins to the galea was performed under local anesthesia. Given local inflammation and uncertain margin status, delayed reconstruction was planned pending histopathological confirmation. After clear margins were verified, controlled subgaleal undermining allowed tension-reduced primary closure. This staged strategy ensured oncologic safety while preserving hair-bearing scalp and avoiding unnecessary flap reconstruction.
Patient medical history
A 48-year-old woman was referred after incomplete excision of a nodular basal cell carcinoma (nBCC) of the anterior scalp performed in private plastic surgery practice. Histology demonstrated tumor involvement of the lateral margins, while the deep margin was free of tumor. Postoperatively, wound rupture and infection developed. Microbiology showed sparse growth of Staphylococcus aureus, and antibiotic therapy was initiated. The patient was otherwise non-smoking and healthy, with well-treated asthma, as her only relevant comorbidity.


Before and After
Patient examination
Clinical examination revealed a 22 × 19 mm anterior scalp defect with limited perifocal erythema and minimal purulent discharge. No regional lymphadenopathy was palpable.
Pre-operative considerations
Initial histopathology demonstrated nodular basal cell carcinoma with focal lateral margin involvement and a clear deep margin, without perineural invasion or other high-risk features. In accordance with current recommendations for low-risk BCC, re-excision with 3 mm clinical margins to the galeal level was planned to achieve oncologic clearance1. Intraoperative frozen section was considered, as margin assessment is often performed prior to flap reconstruction to ensure radical excision before tissue rearrangement. However, given the anticipated large circumferential extent of the scalp excision, frozen analysis would have permitted only partial peripheral sampling and was therefore unlikely to substantially increase oncologic certainty or alter the operative strategy. Definitive paraffin histology was deemed sufficient.
The scalp consists of five layers: the skin (epidermis and dermis), subcutis, galea aponeurotica, loose areolar plane, and pericranium. Due to firm adherence between skin and galea, intrinsic elasticity is limited. Tissue recruitment depends primarily on subgaleal undermining. However, excessive undermining or flap design in previously inflamed tissue increases vascular risk and may create additional alopecic scars.2 In the present case, reconstruction was further complicated by recent infection, local inflammation and uncertain tumor clearance.
For these reasons, delayed closure was intentionally chosen from the outset. Although a local rotation (ying-yang) flap and also skin grafting was considered as reconstructive options, definitive flap reconstruction was deferred until histologic clearance was confirmed. Immediate flap transfer in a field with uncertain margins risks oncologic compromise and unnecessary tissue rearrangement if further re-excision is required.
During the postoperative period and after confirmation of clear margins, progressive tissue relaxation occurred following the initial high-tension wound closure and partial wound dehiscence. This resulted in increased scalp mobility, which allowed renewed subgaleal undermining and ultimately enabled delayed primary closure at the second procedure, thereby avoiding skin grafting or flap reconstruction. Achieving a tension-free closure was prioritized, as excessive wound tension in the scalp is associated with scar widening and secondary alopecia due to mechanical stress and vascular compromise of hair-bearing skin. A rotation (yin–yang) flap was therefore not required. Avoiding flap transposition preserved native hair-bearing scalp, minimized additional scarring, and reduced overall reconstructive morbidity.
Closure orientation was selected to balance biomechanical tension redistribution with preservation of the anterior hairline contour. On the anterior scalp, scar visibility is influenced not only by classical Langer’s lines but also by hair direction and follicular orientation.3

Day of first surgery, 14 days after first examination.
Clinical examination revealed a 22 × 19 mm anterior scalp defect with limited perifocal erythema and minimal purulent discharge. No regional lymphadenopathy was palpable.
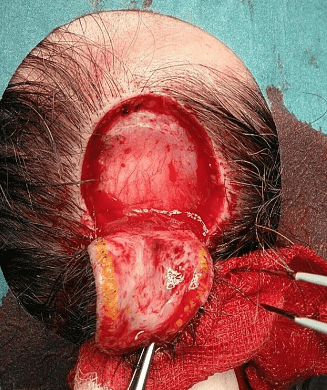
Excision carried down to the galeal level.
Under local anesthesia with lidocaine and adrenaline, re-excision was performed with 3 mm clinical margins to the level of the galea.
Subgaleal undermining to increase advancement.
Controlled lateral undermining was performed in the subgaleal plane to improve tissue mobility and reduce closure tension.
Deep dermal inverted sutures.
Hemostasis was secured. Deep dermal inverted sutures (Vicryl 3-0) were placed to reduce dead space and redistribute tension.
Interrupted Prolene sutures over Spongostan and Jelonet.
Given residual tension and the need to await histopathological confirmation, the wound was provisionally supported with Spongostan and covered with Jelonet. Skin closure was completed using interrupted Prolene 3-0 sutures.

Post-operative day 5.
Histopathological analysis confirmed a diagnosis of nodular basal cell carcinoma with tumor-free margins, both in depth and on all sides (distance not specified).

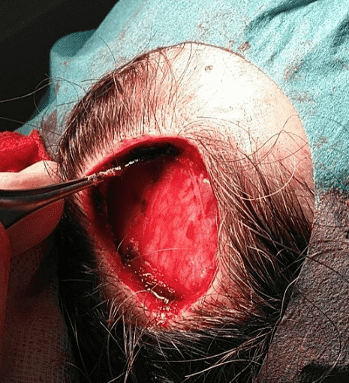
Post-operative day 12 following removal of Spongostan and Jelonet.
Stage 2 was performed 12 days after re-excision. After removal of temporary support material and refreshing of wound edges, controlled subgaleal undermining was again undertaken to optimize mobility.

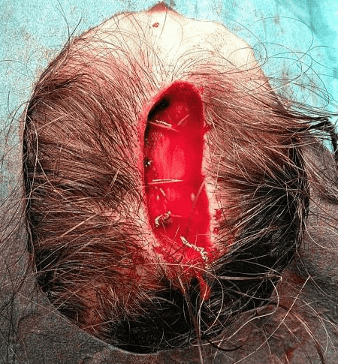
Renewed subgaleal undermining and deep dermal inverted sutures.
After confirmation of clear margins, controlled subgaleal undermining allowed tension-reduced primary closure. A rotation (ying-yang) flap was therefore not required. Avoiding flap transposition preserved hair-bearing scalp, minimized additional scarring, and reduced reconstructive morbidity.

Final wound closure.
Final skin closure was achieved using interrupted and mattress sutures (Prolene 3-0).
Pearls
- In incompletely excised scalp BCC, staged reconstruction enhances oncologic safety.
- Subgaleal undermining is the principal mobilization plane in scalp closure.
- Excision to galeal level improves deep margin control.
- Mattress sutures facilitate tension redistribution and reduce focal ischemia.
- Closure planning must account for both tension vectors and hair orientation.
Pitfalls
- Immediate flap reconstruction prior to margin confirmation may compromise oncologic management.
- Excessive undermining may jeopardize vascularity.
- High-tension closure increases risk of dehiscence and alopecia.
- Neglecting hair direction may result in suboptimal cosmetic outcomes.
Post-operative plan
The patient was discharged on the day of surgery with instructions for routine wound care. Sutures were planned for removal after 10–14 days given the scalp location. Histopathological evaluation of the re-excision specimen was requested to confirm complete tumour clearance. Clinical follow-up was arranged to assess wound healing, scar quality, and potential alopecia, as well as to monitor for local recurrence.
The post-operative photo on day 21, demonstrates a thin scar, with surrounding crust. The anterior hairline is intact. Note that hair in a radius of 1 cm around the excision line was removed prior to surgery for better access, and is expected to grow out.
References
1: Gulleth Y, Goldberg N, Silverman RP, Gastman BR. What is the best surgical margin for a Basal cell carcinoma: a meta-analysis of the literature PRS. 2010 oct.; 126 (4):1222-31
2: Leedy JE, Janis JE, Rohrich RJ. Reconstruction of acquired scalp defects: an algorithmic approach. Plastic and Reconstructive Surgery. 2005;116(4):54e–72e. DOI: 10.1097/01.prs.0000179188.75076.9b
3: Beasley NJ, Gilbert RW. Scalp and forehead reconstruction. Clinics in Plastic Surgery. 2005;32(2):203–215. DOI: 10.1016/j.cps.2004.11.002