Keywords: Basal Cell Carcinoma, Skin Cancer, Eyelid Reconstruction, Tarsoconjuctival flap, Tripier flap.
Authors: Ajla Sabitovic, MD, Rikke Børthy Petersen, MD, Nanja Gotland Sundstrup, MD. Department of Plastic Surgery and Burns Treatment, Copenhagen University Hospital, Rigshospitalet, Denmark.
Abstract
This case describes the use of a tarsoconjuctival flap for reconstruction of the lower eyelid following excision of a basal cell carcinoma in a 76-year-old woman. Due to the tumor size, depth and location near the limbus of the eye, direct closure was not possible. The tarsoconjuctival flap was chosen as the preferred reconstructive approach because of its ability to reconstruct all layers of the eyelid. Postoperative follow-up at six months demonstrated satisfactory aesthetic and functional outcomes.
Patient medical history
A 76-year-old woman presented with a biopsy-confirmed nodular basal cell carcinoma involving the right lower eyelid. Tumor excision was performed in general anesthesia with 3 mm margin and intraoperative frozen-section control, confirming tumor free margins. Resection resulted in a full-thickness defect involving approximately 90% of the lower eyelid. Reconstruction was performed with a tarsoconjuctival flap for the posterior lamella and a Tripier flap from the upper eyelid for the anterior lamella.


Before and After
Patient examination
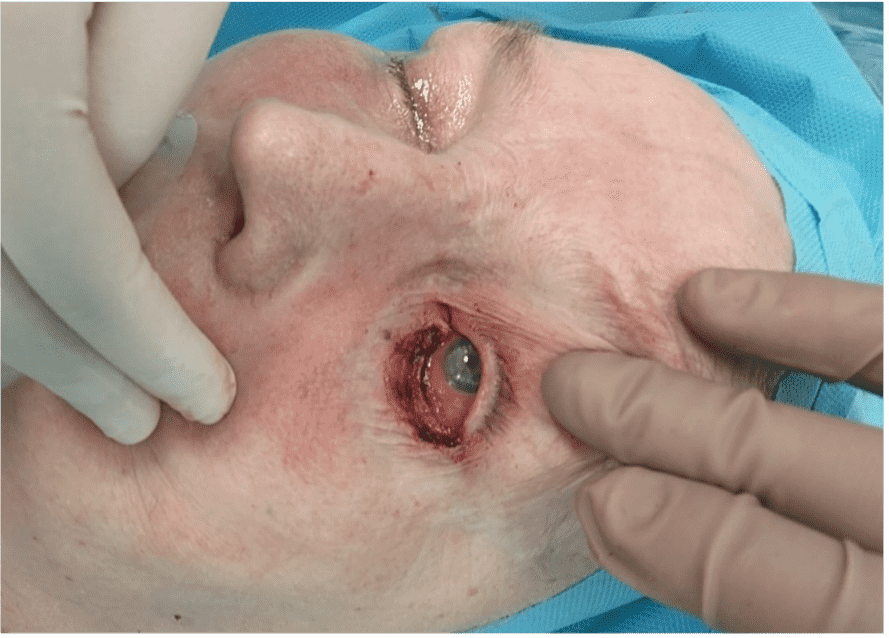
Clinical examination revealed a 12 x 10 mm elevated ulcerating lesion involving the right lower eyelid, extending into conjunctiva and limbus.
Pre-operative considerations
The patient presented with a full-thickness defect of the lower eyelid involving conjunctiva and the inferior eyelid margin. Due to the tumor size and location direct closure was not possible. Reconstruction with a flap was therefore required to secure reconstruction of all layers of the lower eyelid to give the eyelid full support and thereby secure its function.

Step 1
Preoperative skin markings outlining the tumor and 3 mm excision margin.
Step 2
Excision of the tumor was performed with a 3 mm margin, involving the conjunctiva, tarsal plate and lower eyelid skin.

Step 3
The tarsoconjuctival flap was designed and elevated.

Step 4
The flap was transposed to the lower eyelid without traction and inset using absorbable sutures.

Step 5
Reconstruction of the anterior lamella was performed with a Tripier flap designed on the upper eyelid.

Step 6
The flap was elevated as a full-thickness skin graft, including lateral superficial muscle fibers.

Step 7
The flap was transposed without tension to the defect of the lower eyelid.

Step 8
The flap corresponding to the lower eyelid was inset using 6-0 absorbable inverted interrupted sutures and non-absorbable interrupted sutures placed in the skin.

Step 9
The donor site of the upper eyelid was closed with non-absorbable sutures.

Step 10
The postoperative result of a tarsoconjuctival flap for the posterior lamella and a Tripier flap for the anterior lamella.
Pearls
– Intraoperative frozen-section control
– Preservation of adequate tarsal plate
– Precise flap sizing
– Tension-free flap mobilization
– Appropriate timing of flap division
Pitfalls
– Insufficient tarsal tissue within the flap
– Incorrect timing of flap division
– Risk of postoperative complications
Post-operative plan
Division of the tarsoconjuctival flap was performed four weeks after the primary procedure in local anesthesia.
References
Custer, Philip L. M.D., F.A.C.S.; Maamari, Robi N. M.D.. The Köllner Tarsoconjunctival Flap for Lower Eyelid Reconstruction: Historical Perspective and Surgical Outcomes of 140 Cases. Ophthalmic Plastic and Reconstructive Surgery 38(3):p 294-299, May/June 2022. | DOI: 10.1097/IOP.0000000000002099