Keywords: Lower extremity; Orthoplastic Reconstruction; Split flap; microsurgery
Authors: Luisa Lotter¹, Marta Jezierska¹, Ilja W. Käch¹, Volker J. Schmidt¹; ¹Department of Plastic Surgery and Handsurgery, HOCH, Health Ostschweiz, Cantonal Hospital St.Gallen, St.Gallen, Switzerland
Abstract
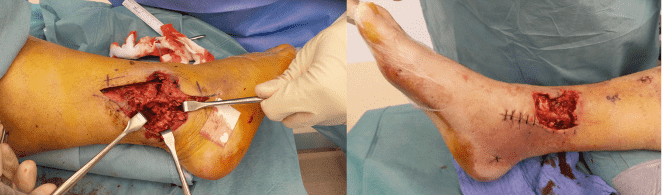
46-year-old man presented with two full-thickness soft-tissue defects of the distal right lower leg (medial 7 × 4 cm, lateral 10 × 5 cm) with exposed tendons, osteosynthesis material, and bone after a Gustilo grade IIIb open tibial and fibular fracture. During initial orthopedic stabilization, interdisciplinary orthoplastic assessment and planning were performed. Because of exposed functional structures and two spatially separated defects with healthy anterior skin between them, microsurgical free-tissue reconstruction was chosen to provide stable coverage while preserving the anterior skin and preventing flap-related functional impairment. Reconstruction was achieved using a split anterolateral thigh (ALT) flap based on two independent perforators, enabling simultaneous coverage of both defects with a single vascular pedicle.
Patient medical history
The patient’s medical history was significant for type 2 diabetes mellitus, two-vessel coronary artery disease, and obesity.

Before and After
Patient examination
- medial defect: 7 × 4 cm with exposed tendons
- lateral defect: 10 × 5 cm with exposed bone and osteosynthesis material
Pre-operative considerations
Reconstruction of distal lower-leg defects with exposed hardware and tendons requires durable vascularized soft-tissue coverage to prevent infection and ensure limb salvage.
The following considerations guided reconstructive planning:
1.tTwo separate defects in close proximity and including the two ankle subunits are associated with functional loss if larger one-flap solutions (e.g., latissimus dorsi) are applied.
2.tPreservation of the intact and functional relevant anterior soft tissue bridge should be taken into consideration
3.tEither two independent flaps (e.g., SCIP or ALT) or a single flap capable of division into multiple components are suitable options.
4.tMuscle flaps are not optimal if further orthopedic interventions are required in the future (lower vascular randomization compared to fasciocutaneous flaps)
5.tThe ALT flap offers a long vascular pedicle, reliable perforators, and sufficient tissue volume while permitting intraflap splitting when multiple perforators are present.
6.tA perforator-based split ALT flap allows simultaneous coverage of spatially separated defects while avoiding multiple donor sites.
7.tRecipient vessel preparation focused on the anterior tibial artery and venae comitantes to ensure reliable inflow and venous drainage.
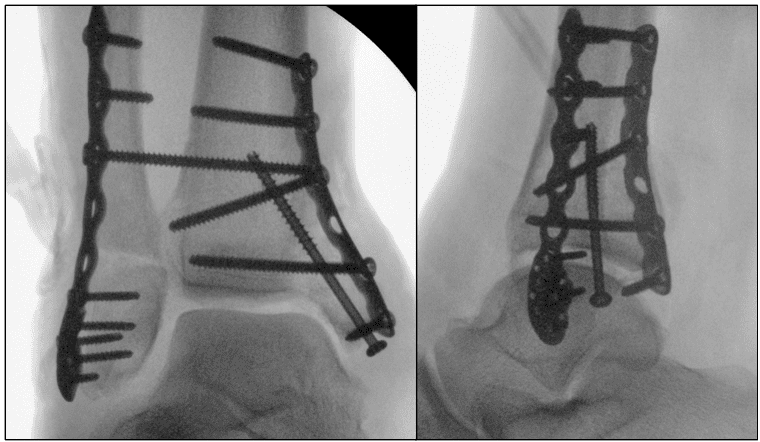
Radical wound bed preparation and hardware assessment
After removal of the negative pressure wound therapy (NPWT) dressing, the wound was thoroughly inspected, radically debrided, and sampled for microbiology. The osteosynthesis material was largely covered except for a small exposed segment. Concurrently, ligamentous and peroneal tendon reconstruction was performed to restore ankle stability. This ensured an adequately conditioned wound bed and a stable biomechanical environment prior to definitive microsurgical soft-tissue coverage.
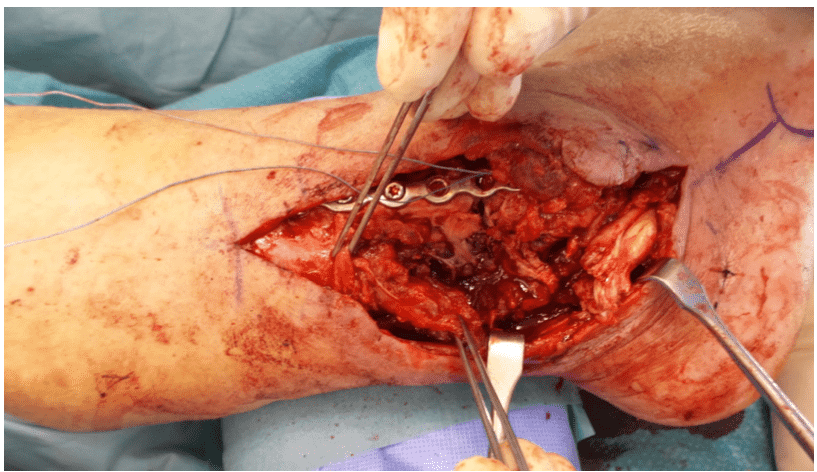
Preparation of the recipient site
Concurrently, ligamentous and peroneal tendon reconstruction was performed to restore ankle stability. Through an anterior longitudinal approach, the anterior tibial artery and its concomitant veins were identified and mobilized over a length of approximately 6 cm. Side branches were clipped, and the vessels were prepared for subsequent microsurgical anastomosis.
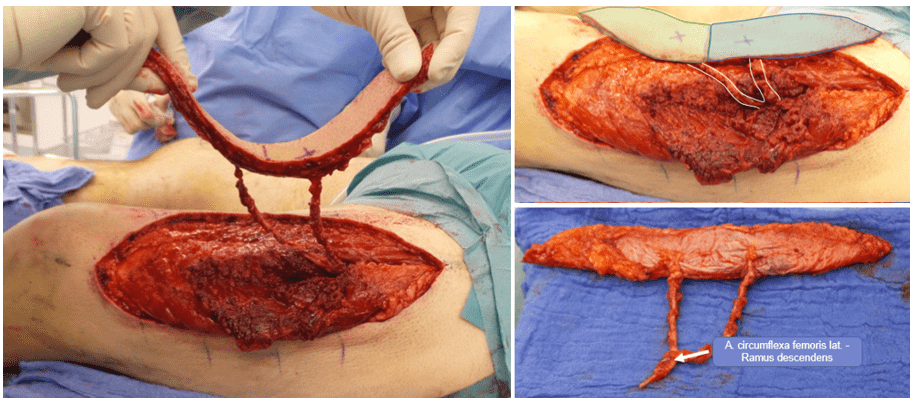
Flap dissection
Simultaneously, a bipedicled anterolateral thigh (ALT) flap was harvested from the left thigh. The flap design was centered over the two dominant perforators to allow subsequent division into two equally sized skin islands (marked in green and blue). After fascial incision, two robust perforators with a long intramuscular course (approximately 12 cm) were identified.
The descending branch of the lateral circumflex femoral artery was dissected proximally to achieve adequate pedicle length and vessel caliber. Prior to flap transfer, perfusion of both distal flap segments was confirmed using indocyanine green angiography.
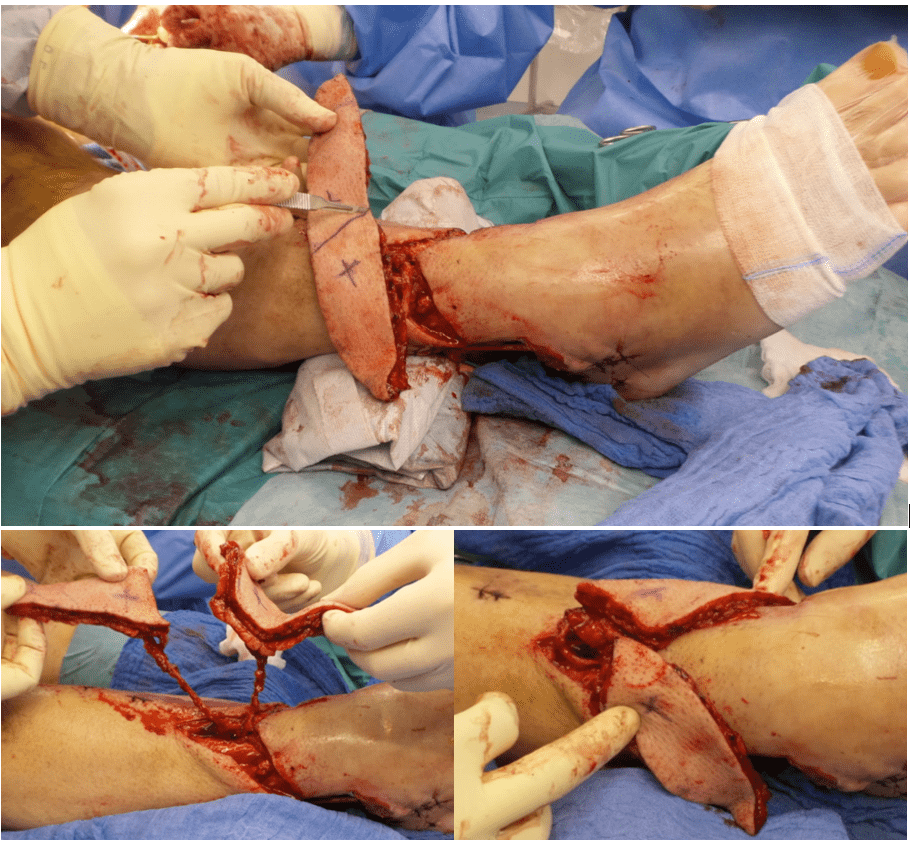
Microsurgical anastomoses and flap splitting
The pedicled flap was transferred to the lower-leg defect without torsion. Venous anastomoses were performed using a 2.0-mm coupler and an additional hand-sewn anastomosis to the two venae comitantes. An end-to-side arterial anastomosis to the anterior tibial artery was completed using interrupted microsurgical sutures (Dafilon 8-0). After systemic heparinization and clamp release, the flap demonstrated immediate and stable perfusion. The anastomotic site was reinforced with fibrin sealant.
The flap was subsequently divided between the two perforators, creating two spindle-shaped skin islands. One island was inset into the medial defect, whereas the second island was rotated to cover the distal lateral defect. Care was taken to avoid torsion or traction on both pedicles during inset.
Flap inset
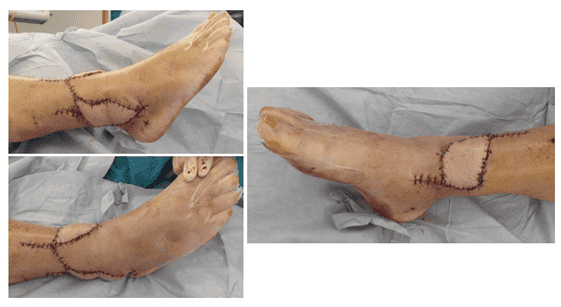
Both flaps were trimmed and inset tension-free using interrupted sutures. Final inspection confirmed excellent perfusion of both components. The donor site was reconstructed with a partial resorbable mesh reinforcement of the fascial defect and primary skin closure with drainage.
Follow-up 3 months
Follow-up with full healing.
Pearls
- A perforator-based split ALT flap enables simultaneous subunit reconstruction of multiple adjacent lower-leg defects using a single vascular pedicle.
- Split ALT flaps can preserve healthy and functional relevant skin territories that were in former times often covered with larger and bulky muscle flaps
- Split flaps for multiple and distant lower extremity defect reconstructions with an end-to-site arterial anastomosis pattern enable optimal preservation of the distal extremity vessel axis
- A careful colour duplex examination for perforator localization is ideally performed by the surgeon one day before the operation the final flap design should locate each perforator after division of the flaps at the transition from the proximal to the middle third of the flap
- Intraoperative ICG-perfusion mapping should be used to minimize the risk of distal flap necrosis
- Documentation of the flap rotation ankle and direction (clockwise or anticlockwise) for each pedicle within the operation report is crucial, if revision surgery is required.
- Embedding the pedicels into fibrin glue minimizes the risk for pedicle torniquet and tension.
Pitfalls
- A lack of sufficient independent perforators during the colour duplex examination demands an alternative reconstructive plan (e.g. two separate flaps of split latissimus dorsi flap in this case)
- Distal lower-leg reconstruction requires meticulous preparation of recipient vessels, as vessel quality may be compromised after severe trauma. In older patients (>50y) and in younger patients with a risk profile for atherosclerosis an adequate recipient vessel assessment should be performed (e.g. CT- or MR-angiography).
- Lower extremity traumas are associated with a significant rate of clinically occult deep vein thrombosis. The vascular examination should be generously supplemented with an assessment of the deep venous system in case of suspicion.
- Excessive tension or pedicle twisting during rotation of split skin islands can lead to vascular compromise.
- Progressive tunnelling of the pedicle/s should be avoided if secondary edema or swelling is likely.
Post-operative plan
- Strict limb elevation and bed rest were maintained for five postoperative days. Flap perfusion was monitored hourly for the first 24 hours and at regular intervals thereafter.
- A structured dangling protocol was initiated from postoperative day 5 to gradually condition venous outflow.
- The patient was immobilized in a custom splint with protected partial weight-bearing of 15 kg for six weeks due to the underlying osteosynthesis. A pressure-relieving recess was incorporated over the flap to avoid compression and prevent equinus deformity.
- Low-molecular-weight heparin anticoagulation and intravenous antibiotics were administered according to institutional microsurgical protocol and adjusted to microbiological results.
- Compression therapy was continued for six months, with scheduled outpatient follow-up at regular intervals.
References
Donor site in anterolateral thigh (ALT) free flaps: A systematic review of closure techniques and introduction of a management algorithm Chang, Chad et al. Journal of Plastic, Reconstructive u0026 Aesthetic Surgery, Volume 105, 243 – 259
Split anterolateral thigh free flaps for bilateral open fracture ankle defects: A one donor, two flap solution, Wilson, Elizabeth et al. JPRAS Open, Volume 46, 2025, Pages 61-64