Keywords: Tennessee flap, modified C-H flap, nipple reconstruction, invasive ductal carcinoma, DIEP flap, secondary breast reconstruction
Authors: Mikkel Halborg Sørensen, MD; Nanja Gotland Sundstrup, MD; Christian Lyngsaa Lang, MD Institution: Department of Plastic Surgery and Burns, Rigshospitalet, Copenhagen University Hospital, Denmark
Abstract
A 50-year-old woman with a history of invasive ductal carcinoma (IDC) underwent right-sided papilla reconstruction following secondary deep inferior epigastric perforator (DIEP) flap breast reconstruction. A Tennessee flap technique was used in conjunction with correction of lateral volume of the DIEP flap. The technique provided projection and predictable positioning relative to the contralateral nipple-areola complex. The procedure was performed under local anesthesia in an outpatient setting. The immediate postoperative appearance was satisfactory, and wound healing proceeded without complications. This case higlights the continued utility of the Tennessee flap as a simple, safe, and reproducible technique for delayed nipple reconstruction.
Patient medical history
A 50-year-old woman with a history of IDC underwent right-sided subcutaneous mastectomy in 2017. In 2025, she underwent unilateral delayed autologous breast reconstruction using a DIEP flap. In 2026, completion of the reconstructive process was planned with papilla reconstruction. The patient was in good general health, non-smoking, and without known comorbidities.
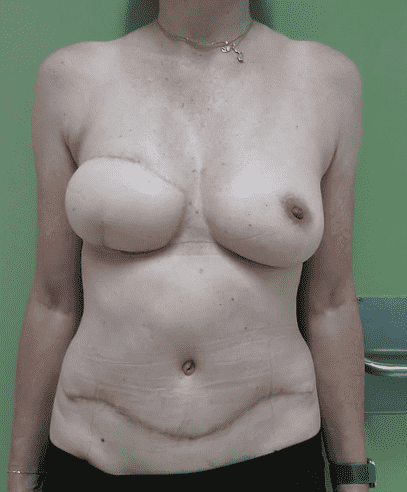
Before and After
Patient examination
Clinical examination demonstrated a well-integrated right-sided DIEP flap, good symmetry compared to the contralateral breast, even though the flap was too voluminous at the lateral side. Absence of nipple-areola complex (NAC) on the reconstructed side and a contralateral areola with soft and not sharply demarcated borders. A well-healed lower abdominal donor-site scar from the DIEP flap harvest was present.
Pre-operative considerations
In Denmark, the Tennessee flap, a modification of the classic C-H flap (named for its C- and H-shaped incision pattern), is frequently used for nipple reconstruction.1 It is a random-pattern dermal flap valued for its simplicity, reproducibility, and suitability for outpatient surgery under local anesthesia. Unlike graft-augmented techniques, projection is achieved solely through folded dermis, rendering long-term nipple height dependent on scar maturation and dermal remodeling. Intraoperative overcorrection of nipple projection by approximately 20–30% is therefore recommended, as projection loss up to 38 % has been reported at one year.2 In the present case, the DIEP flap skin envelope was soft and pliable. These factors reduced the risk of vascular compromise and excessive fibrosis. The lateral fullness allowed for simultaneous contour refinement without altering central flap perfusion.
The Tennessee flap consists of a centrally based rectangular dermal segment with two lateral wings. The central limb forms the core of the neo-papilla, while the wings provide circumferential support. Elevation is performed in the subdermal plane with preservation of dermal thickness to maintain perfusion from the subdermal plexus. In DIEP-flap reconstructed breasts, excessive undermining should be avoided to protect perforator-dependent perfusion.
Projection is achieved by folding the central limb and approximating the lateral wings with deep dermal sutures, thereby creating a scar-supported dermal cylinder without internal reinforcement. Tension-free closure is essential, as circumferential compression accelerates projection loss. Although the technique produces two adjacent scars and gradual shrinkage over time, these were considered acceptable in this case and are expected to be camouflaged by subsequent areola tattooing. Nipple position was determined with the patient in the standing position using a temporary nipple template to achieve optimal three-dimensional symmetry with the contralateral breast.
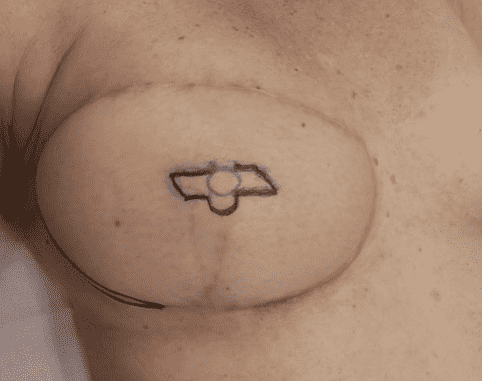
Pre-operative markings
- The lateral excision and contouring of the DIEP flap.
- The Tennessee flap design for papilla reconstruction

Local anesthesia was administered.
Local anesthesia was administered using lidocaine.

Incision of the Tennessee Flap
The flap incisions were performed according to the marked design

Initial flap elevation.
Initial elevation of the dermal flaps was performed in the subdermal plane.

Elevation with Preservation of Dermal Thickness
Further flap elevation was performed while preserving dermal thickness to maintain vascularity from the subdermal plexus.
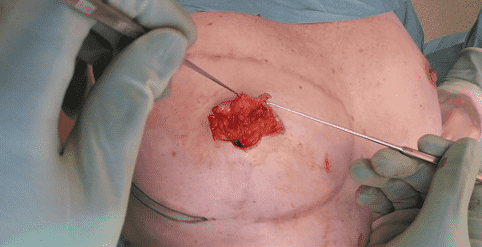
Completed Flap Mobilization
The dermal flaps were fully elevated and mobilized in preparation for formation of the neo-papilla.
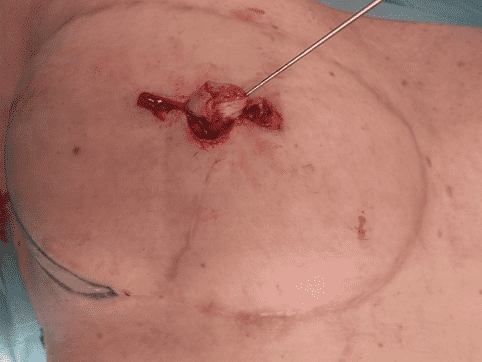
Creation of Nipple Projection
The central limb of the flap was folded to initiate projection of the reconstructed papilla.
Shaping of the Neo-Papilla
The lateral wings were wrapped around the central limb and secured with sutures to shape the neo-papilla, followed by skin closure.

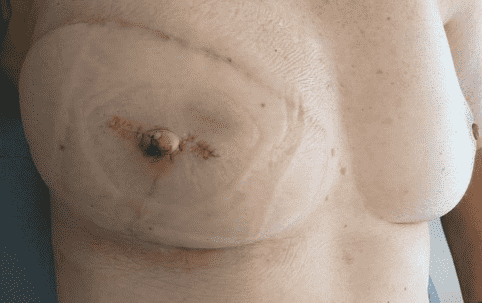
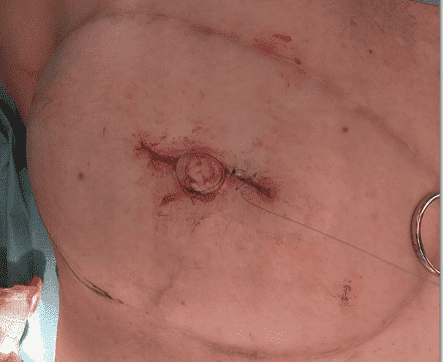
Immediate Postoperative Result
Immediate postoperative appearance following papilla reconstruction.
Pearls
Determine nipple position with the patient upright.
Overcorrect projection of the nipple intraoperatively (up to 20–30%) to compensate for predictable long-term contraction and dermal remodeling.
Preserve maximal dermal thickness during flap elevation to maintain subdermal plexus perfusion and structural rigidity of the neo-papilla. Flap base width must be sufficient to preserve random-pattern perfusion.
Minimize circumferential skin tension at closure, as external compressive forces accelerate projection loss.
Perform simultaneous minor contour corrections cautiously, ensuring they do not compromise the vascular base of the flap.
Planned areola tattooing reduces the visual impact of adjacent scars.
The flap should be designed away from prior scar lines to avoid compromised microvascularity.
Pitfalls
- Long-term loss of projection due to flap contraction should be anticipated.
- The height of the neo-nipple may initially be adequate for symmetry, but over time can shrink.
- Flap design too close to previous scars may compromise vascularity.
- Inadequate patient counseling regarding expected projection loss may result in dissatisfaction.
- Flap on flap, important to ensure dimensions to supply sufficient dermal perfusion.
Post-operative plan
Dressing removal and suture removal at postoperative day 7–10. Clinical evaluation of projection and wound healing. Areola tattooing planned after complete healing, typically 3 months. Final evaluation at 3 months to assess projection maintenance and symmetry.
At suture removal 10 days post-operative (picture), healing was uneventful. The papilla maintained adequate projection with no signs of ischemia or wound complications.
References
1. Yoo H, Park S, Chang H. Nipple reconstruction using modified C-V flap with purse-string sutures for maintenance of long-term nipple projection. Journal of Plastic, Recon-structive and Aesthetic Surgery. 2023;84:62-70. doi:10.1016/j.bjps.2023.04.061
2. Yoon JS, Chang JW, Ahn HC, Chung MS. Modified C-H flap for simultaneous nipple reconstruction during autologous breast reconstruction: Surgical tips for safety and cosmesis. Medicine (United States). 2018;97(38). doi:10.1097/MD.0000000000012460