Keywords: Goldilock, Mastectomy, Goldilocks mastectomy, Breast reconstruction, mamma reconstruction, Oncoplastic, Risk reducing mastectomy, breast cancer, cancer
Authors: Nanja Gotland Sundstrup (MD), Pia Cajsa Leth Andersen (MD) Institution: Department of Plastic Surgery and Burns, Rigshospitalet, Copenhagen University Hospital, Denmark
Abstract
This case report describes the “Goldilocks procedure” as a technique used for primary breast reconstruction in a patient with prior bilateral c. mamma, treated with lumpectomy and radiotherapy. An implant-based reconstruction was not advised due to the radiotherapy, and she was reluctant to undergo larger scale autologous reconstruction. She was suggested the “goldielocks procedure” as an upgrade to the simple mastectomy which was her alternative consideration. the Goldilocks procedure has the advantage of achieving immediate formation of a small breast, while simultaneously establishing a favorable platform for potential delayed reconstruction with autologous fat grafting.
Patient medical history
The patient, a 67-year-old woman had a history of bilateral breast cancer: left-sided in 2016 and right-sided in 2023, treated with lumpectomy, and radiotherapy, with additional chemotherapy for the right-sided cancer. Further she was found to carry a pathogenic CHEK2 mutation. The patient underwent bilateral risk reducing mastectomy using the Goldilocks technique, with maximal preservation of the skin envelope and subcutaneous tissue (1). Compared with a simple mastectomy, this approach preserved a good shape and projection resulting in the formation of a small breast. Furthermore, the result provided a more favorable foundation for potential delayed breast reconstruction. The patient was planned for a reconstruction in terms of lipofilling, and mastopexy as well as nipple reconstruction.

Before and After
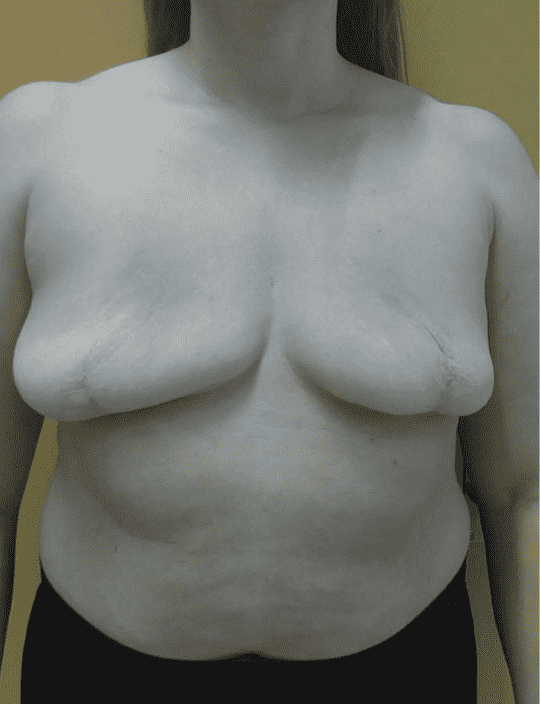
Patient examination
The patient generally presented with good skin quality. Clinical examination revealed sequelae of prior breast surgery, including lumpectomy scars bilaterally; on the left side laterally, on the right side periareolar accompanied by skin retraction in the inferomedial quadrant of the breast.
Pre-operative considerations
To minimize the risk of breast cancer, a bilateral risk-reducing mastectomy was indicated. Several surgical techniques were considered, including simple mastectomy; however, the patient expressed a desire to retain a small breast volume without undergoing major reconstructive procedures such as free flap reconstruction. Furthermore, given the patient’s history of prior radiotherapy, implant-based reconstruction was deemed undesirable. Consequently, the Goldilocks mastectomy technique was selected. This approach allowed reconstruction of the cutaneous envelope to form a small breast mound while preserving maximal skin, thereby providing an optimal foundation for subsequent reconstruction with autologous fat grafting.
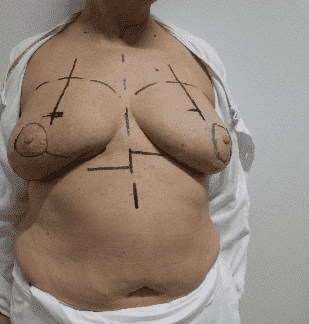
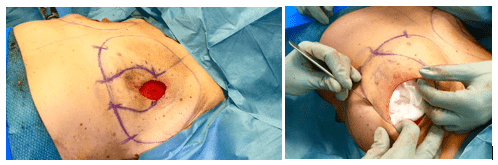
Pre-operative markings
Preoperative markings were performed with the patient upright. The upper breast border, breast footprint, and the inframammary fold (IMF) were delineated, and the median marked from the upper breast boarder extending inferiorly. The planned neo-papilla position was placed on the meridian 8 cm inferior to the upper breast border, with an additional reference point 10 cm lateral to the thoracic midline beneath the breast. As the mastectomy included excision of the native NAC, periareolar incision lines were used.
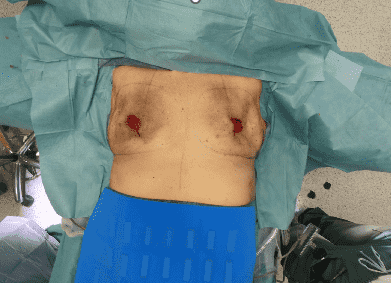
Skin envelopes after subcutaneous mastectomy
The subcutaneous mastectomy was performed, resulting in well perfused skin envelopes bilaterally. The hyperpigmentation of the skin is residual from the radiotherapy.
Markings for de-epithelialization
The skin was folded to preserve the maximal amount of tissue for de-epithelialization and temporarily secured with staples. The area designated for de-epithelialization was marked from the point of the planned neopapilla 8 cm below the upper breast border at the breast meridian, extending to the inframammary fold (IMF).
The skin ready for de-epithelization
The breast was stuffed with napkins to help stretching the skin for easy de-epithelization.

After De-epithelialization

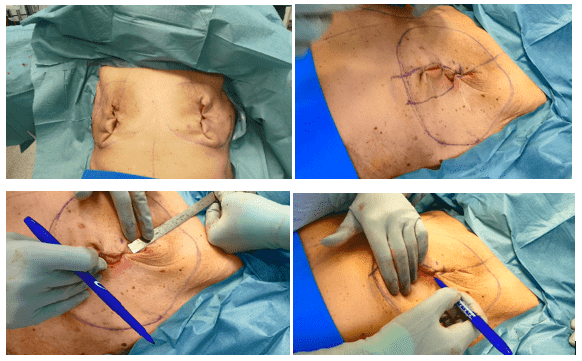
Mobilization of de-epithelialized flaps
An incision was made through the dermis and subcutaneous tissue along the medial line vertically and horizontally through the inframammary fold.
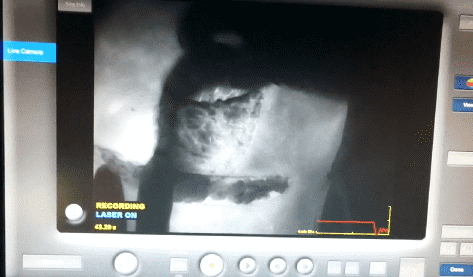
Fluorescence imaging
Skin perfusion was checked, to secure vital skinflaps by using fluorescence imaging.
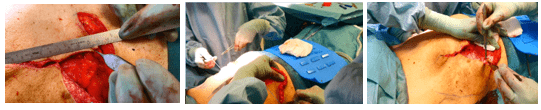
Adjusting lateral boarder
The lateral excision line was adjusted to the medial side, leading to a marking at 10 cm distally from the top of the vertical line. From this point, a horizontal line was drawn toward the inframmary fold, following a wise-pattern design, to guide further de-epithelialization.
Closure of vertical incisions
When satisfied with the tension of the skin the vertical incisions were closed.
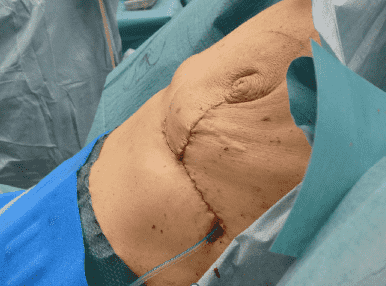
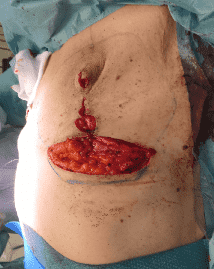
Closure of horizontal incisions
A drain was installed and the horizontal line closed. All sutures were biosyn 4-0, an absorbable suture.
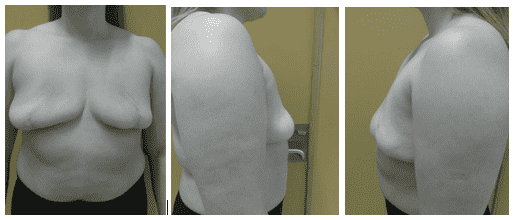
One Year postoperative follow-up
At one-year postoperative follow-up, the patient have had one time lipofilling and she is scheduled for a second lipofilling and mastopexy/ nipple reconstruction.
Pearls
- This technique is straightforward and well-suited for patients desiring a smaller autologous reconstruction and prefer to avoid extensive reconstruction, The best results are obtained in women with preoperative larger breasts, but can be considered for all breast sizes, if the patient is well informed of the expected result with a smaller breast.
- This technique can easily be combined with secondary autologous fat grafting to increase breast volume and improve shape.
- Additionally, the technique can be relevant in cases where it is unknown at the time for mastectomy if the patient would need postoperative radiation. In such a case the preservation of the skin envelope, and no need for postoperative radiation, would create the possibility for delayed implant-based reconstruction.
Pitfalls
- Communication with the patient is vital. She must be thoroughly informed about the result after a goldielock procedure, meaning that the result is a smaller and deflated breast, not necessarily pleasing to the eye. The Goldilocks mastectomy alone is insufficient for patients desiring a moderate-large size breast. It is an option that provides more than a mastectomy, and less than any other reconstruction. But in the right situations – it is just right for the patient.
Post-operative plan
- Drains were removed 2 days postoperatively, once the output was serous and less than 30 mL per 24 hours.
- The patient was instructed to wear a surgical bra continuously (day and night) for the first 3 weeks, followed by daytime use for the subsequent 3 weeks.
- A follow-up evaluation with the operating surgeon were scheduled at three months to assess the long-term aesthetic outcome and determine the need for potential secondary autologous fat grafting.
References
1) Richardson H, Ma G. The Goldilocks mastectomy. International Journal of Surgery. 2012 vol. 10 issue 9 p. 522-26