Keywords: Nail removal, nail bed biopsy, nail punch biopsy, Subungual Melanoma
Authors: Linnea Kristensen Ejiofor, MD, Department of Plastic Surgery and Burns Treatment, Copenhagen University Hospital, Rigshospitalet, and Magnus Balslev Avnstorp, Specialist plastic surgeon, Zealand University Hospital, Roskilde.
Abstract
Nail changes can reflect a wide spectrum of benign and malignant conditions, making accurate clinical evaluation essential. This case report reviews key background knowledge on common nail alterations and their differential diagnoses. It aims to support clinicians in recognizing when a nail biopsy is indicated and outlines practical considerations for performing the procedure. In addition, the report describes essential steps in the biopsy technique and provides guidance on appropriate postoperative management and follow-up.
Patient medical history
A 72-year-old man was referred to the department of plastic surgery and breast surgery at Zealands University Hospital, Roskilde, on suspicion of malignant melanoma under the nail of his right thumb.


Before and After
Patient examination
The patient presented with hutchinson’s sign, longitudinal melanonychia and no swollen lymphnodes. He had no first-degree relatives with melanoma, no prior history of melanoma (invasive or in situ) and no prior history of other skin cancers.
Pre-operative considerations
- Pigmented longitudinal lesion in the direction of nail growth (melanonychia) with atypical features
- Hutchinson’s sign (pigment lesion in the periungual skin)
- Rapidly growing pigmented nail lesion or nevus
- Suspicion of malignancy following dermoscopic evaluation
- Insufficient diagnostic certainty using non-invasive methods
- Subungual hematoma (trauma-related)
- Onychomycosis (fungal infection)
- Melanocytic hyperplasia (brown, pigmented spots or bands)
- Pyogenic granuloma
- Glomus tumor
- Subungual exostosis
- Myxoid pseudocyst
- Malignant conditions:
- Subungual melanoma
- Squamous cell carcinoma (SCC)
- Document the appearance and width of the pigmented band and the presence or absence of Hutchinson’s sign.
- Perform dermoscopy to evaluate the pigment pattern and exclude benign causes.
- Use ultrasound gel rather than alcohol under the dermatoscope.
- Record relevant history, including trauma, dermatologic conditions, or family history.
- Inform the patient about the risk of nail dystrophy and possible permanent nail loss.
- Ask for local anesthesia without epinephrine.
- Ensure hemostasis using a tourniquet.
- Select the biopsy site at the proximal origin of the pigmentation within the nail fold.
- Consider suturing defects > 3 mm to optimize cosmetic outcomes.
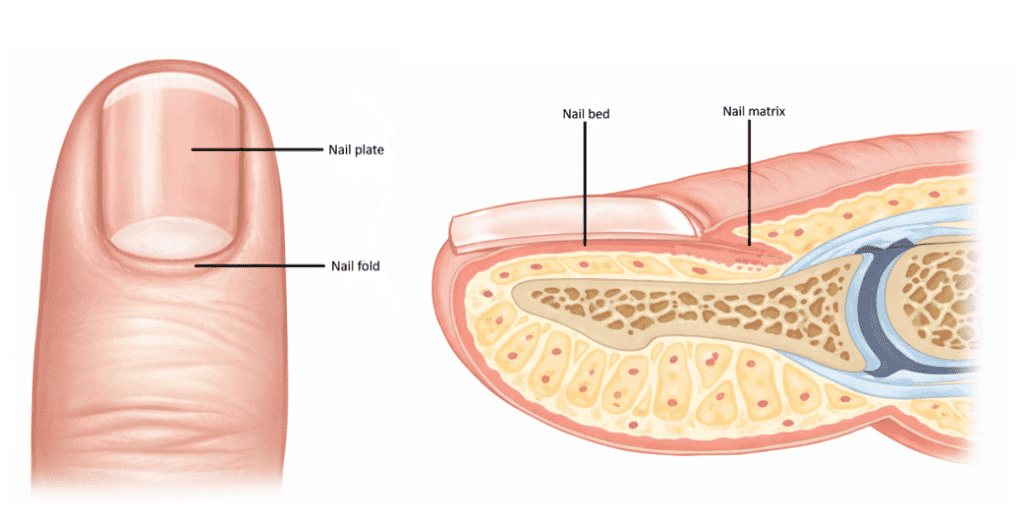
Nail anatomy
- Nail matrix: Growth zone of the nail plate.
- Nail bed: Underlying tissue securing the nail plate to the finger.
- Nail plate: Keratinized structure forming the visible part of the nail.
- Nail folds (cuticle/eponychium): Surrounds the nail plate and protect against infection.
Skin antisepsis and digital nerve block
- Preoperative skin antisepsis.
- Sterile draping (consider a surgical fenestrated drape).
- Perform a digital nerve block at the base of the affected finger or. toe.
Tourniquet
Prepare the tourniquet by cutting into the finger of a surgical glove proximally and distally.

Applying the tourniquet
Apply a proximal tourniquet

Prepare the incision to the nail fold
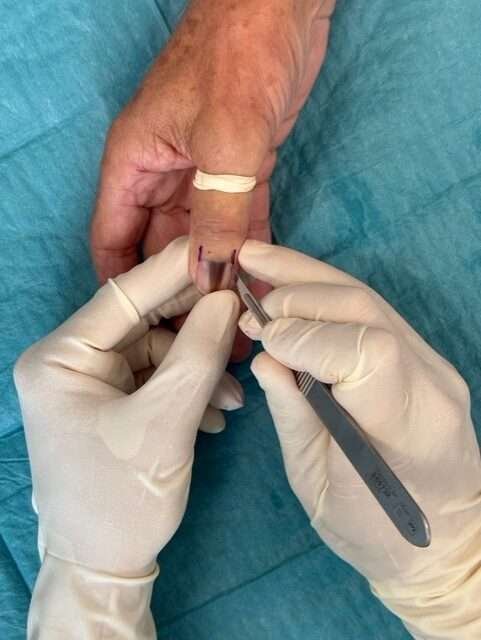
Incision to the nail fold
- Confirm adequate anesthesia.
- Incise the nail fold on both sides of the pigmentation.
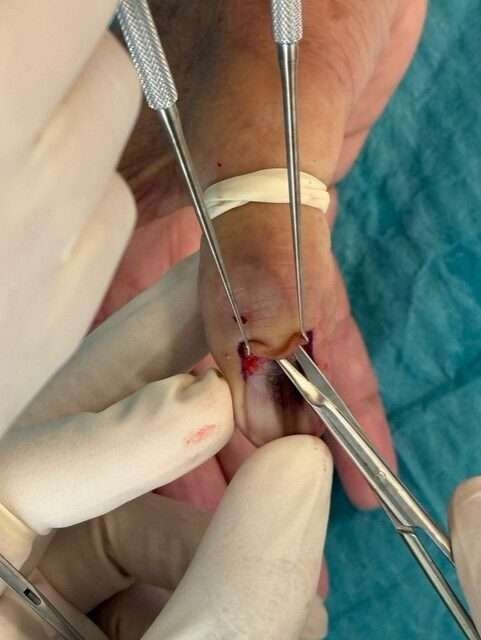
Undermining the nail fold
Undermine the nail fold to visualize the pigmented tissue using first a scalpel and then dissection scissiors.
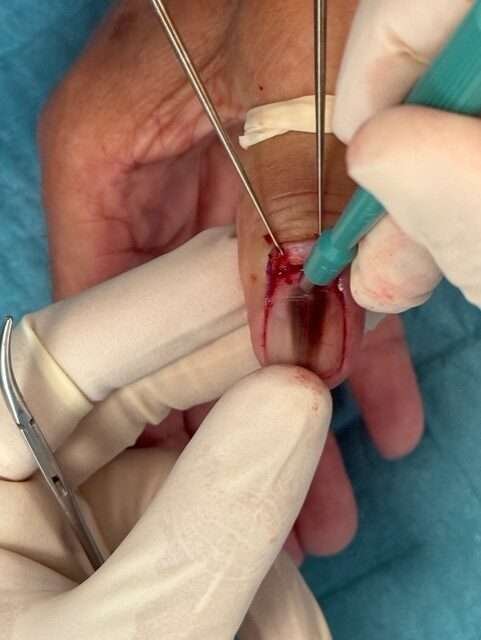
Telescopic Biopsy Technique – punch biopsy through the nail plate
- A punch biopsy (preferably 3–4 mm) can be performed with or without removal of the nail plate. If the punch biopsy is performed without nail plate removal, then it is performed as shown below. Press down to the periosteum at the origin of pigmentation.
- Submit the nail plate, biopsy specimen, and any intervening tissue separately in separate pathology specimen containers and send to pathology.
- Achieve hemostasis.

Nail Plate Removal
- Grasp the free edge of the nail plate with a hemostat and avulse the nail plate with a twisting motion.
- If difficult to detach, perform blunt dissection using a curved dissection scissor beneath the nail plate along the nail groove.
- Submit the nail plate, biopsy specimen, and any intervening tissue separately to pathology.

Nail Bed Biopsy
When the nail plate is removed, a punch biopsy (preferably 3–4 mm) can be performed down to the periosteum at the origin of pigmentation.

Nail bed after biopsy
Achieve hemostasis.

Prepare nail splint
Trim a syringe barrel (typically 10 mL for fingers and toes 2–4; 20 mL for the great toe) to match the size of the nail bed, ensuring smooth, rounded edges.

Adjust the nail splint to detached nail plate

Prepare the nail splint for suture
Create two holes at the proximal end using a needle.

Secure the nail splint
Secure the customized nail splint to the nail fold using 4-0 Nylon sutures through the two holes.

Suture the nail fold
Suture the incisions to nail fold with 4-0 Nylon sutures.

Wound dressing
Apply sterile dressing. For instance, a protective finger dressing or a gauze secured with micropore tape over the nail bed.
Pearls
Pitfalls
Post-operative plan
- Keep the area clean and dry.
- Apply sterile dressing and change as needed.
- Remove sutures and the temporary nail substitute after 14 days.
- Provide instructions regarding signs of infection and bleeding.
- Communicate histopathological results when available.
References
Haneke E. Anatomy of the nail unit and the nail biopsy. Semin Cutan Med Surg. 2015;34(2):95-100
ollina U, Nenoff P, Haroske G, Haenssle HA. The diagnosis and treatment of nail disorders. Dtsch Arzteblatt Int. 2016;113(29-30):509-18.
Singal A, Bisherwal K. Melanonychia: etiology, diagnosis, and treatment. Indian Dermatol Online J. 2020;11(1):1-11
Perrin C, Michiels JF, Boyer J, Ambrosetti D. Melanocytes pattern in the normal nail, with special reference to nail bed melanocytes. Am J Dermatopathol. 2018;40(3):180-1
Agner T, Jensen AN, Sachs C. Negleforandringer, 2020. https://www.sundhed.dk/sundhedsfaglig/laegehaandbogen/hud/symptomer-og-tegn/negleforandringer/ (22. jun 2022).
Agner T, Jensen AN, Sachs C. Paronychion, 2021. https://www.sundhed.dk/sundhedsfaglig/laegehaandbogen/hud/tilstande-. 11
Littleton TW, Murray PM, Baratz ME. Subungual melanoma. Orthop Clin North Am. 2019;50(3):357-366
Jellinek N. Nail matrix biopsy of longitudinal melanonychia: diagnostic algorithm including the matrix shave biopsy. J Am Acad Dermatol. 2007;56(5):803-10
Moossavi M, Scher RK. Complications of nail surgery: a review of the literature. Dermatol Surg. 2001;27(3):225-8.