Keywords: Limb salvage, free flap, anterolateral thigh flap, vastus lateralis, brachial artery injury, Gustilo–Anderson IIIC, microsurgery, trauma reconstruction
Authors: Dr. Ibrahim Güler, Prof. Dr. Cenk Demirdöver. Department of Plastic, Reconstructive and Aesthetic Surgery, Dokuz Eylül University, Izmir, Turkey; Department of Plastic, Aesthetic and Hand Surgery, Otto von Guericke University, Magdeburg, Germany
Abstract
A 16-year-old female sustained a crush injury of the left upper extremity, resulting in an open humeral fracture (Gustilo–Anderson IIIC), brachial artery injury, and extensive soft-tissue loss. Initial treatment by trauma and vascular surgery included external fixation and brachial artery reconstruction using a saphenous vein graft. Early graft thrombosis led to critical limb ischemia, and above-elbow amputation was proposed. An emergency limb salvage attempt was performed using a combined free vastus lateralis and anterolateral thigh flap. The limb was successfully salvaged, with a favorable contour and good long-term functional outcome after secondary debulking procedures.
Patient medical history
A 16-year-old previously healthy female sustained a crush injury to the left upper extremity, resulting in an open humeral fracture (Gustilo–Anderson IIIC), brachial artery injury, and extensive soft-tissue loss [1,2]. Initial management by the trauma and vascular surgery teams at the same hospital included external fixation to stabilize the humeral fracture and reconstruction of the brachial artery using a saphenous vein interposition graft. Early thrombosis of the vein graft led to critical limb ischemia, and above-elbow amputation was subsequently proposed.


Before and After
Patient examination
On examination by the plastic surgery team, the left upper extremity showed extensive soft-tissue loss around the elbow and proximal forearm, with the humerus stabilized in an external fixator. Despite the thrombosis of the brachial artery interposition graft, the hand was still warm with delayed but present capillary refill, indicating residual distal perfusion through collateral arterial flow.
Pre-operative considerations
After early thrombosis of the saphenous vein interposition graft, the limb fulfilled the criteria of a mangled extremity with major vascular injury, open fracture, and extensive soft-tissue destruction. According to institutional trauma algorithms and established trauma scoring systems used in severely injured patients, the extremity was considered to carry a very high risk of limb loss and systemic morbidity, and above-elbow amputation was therefore proposed by the trauma and vascular surgery teams [3,4].
However, in view of the preserved distal perfusion, the patient’s young age, absence of comorbidities, and the presence of viable tissue, a limb-salvage strategy was considered technically feasible by the plastic surgery team. An emergency microsurgical reconstruction using a combined free vastus lateralis and anterolateral thigh flap was therefore selected to preserve the extremity and its function.

Step 1 Radical debridement: Extensive debridement of all non-viable soft tissue exposing the humerus, muscles, and vascular structures.
All necrotic tissue was excised until viable bleeding muscle and soft tissue were reached. The wound was converted into a clean, reconstructable defect measuring approximately 19 x 12 cm.

Step 2 Identification of recipient vessels: Exploration of the proximal arm and elbow region to identify suitable recipient vessels.
The thrombosed saphenous interposition graft was confirmed. Recipient arteries and veins suitable for microvascular anastomosis were identified proximally in the arm.
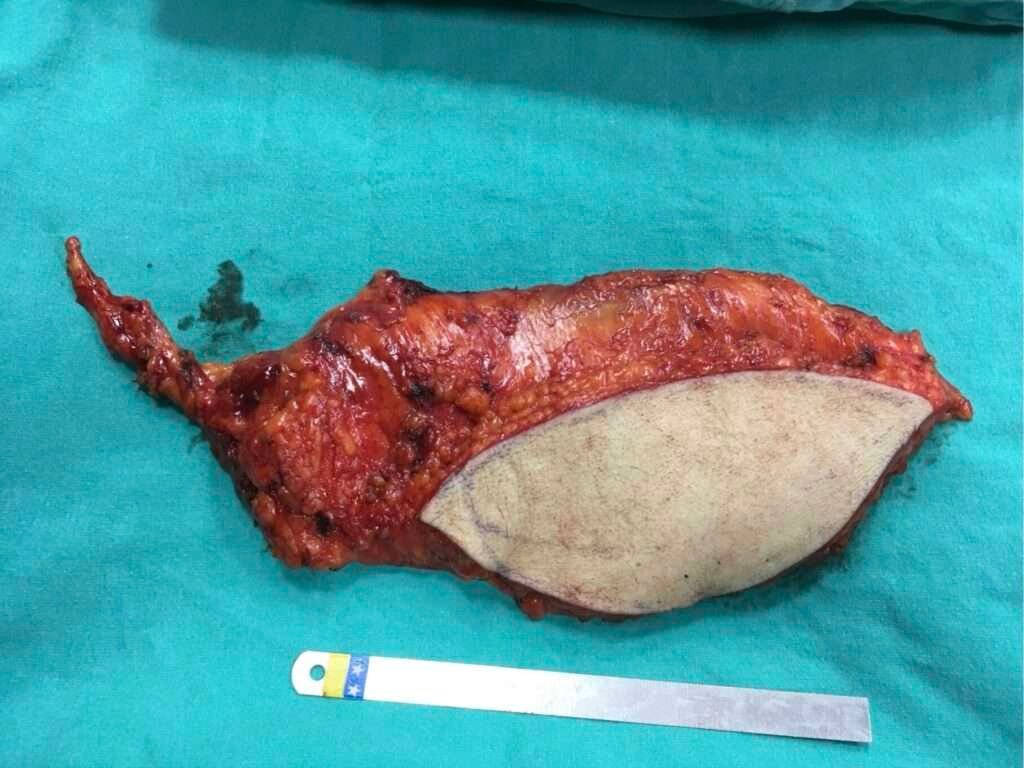
Step 3 Flap harvest and transfer: Combined anterolateral thigh flap including vastus lateralis muscle harvested and prepared for transfer.
A free anterolateral thigh (ALT) flap incorporating a segment of the vastus lateralis (VL) muscle was harvested to provide sufficient tissue volume for reconstruction of the deep soft-tissue defect. After completion of flap harvest, the flap was transferred to the left upper extremity. The thrombosed saphenous vein graft was removed and the recipient vessels were irrigated with heparinized solution, after which a flow-through arterial anastomosis was created between the proximal and distal segments of the brachial artery, with two concomitant veins anastomosed for venous outflow. This was followed by insetting of the vastus lateralis muscle to fill the deep defect and positioning of the ALT skin paddle for definitive surface coverage. The remaining skin defect was covered with split-thickness skin graft harvested from the thigh region.

Early postoperative Result: Early postoperative appearance of the reconstructed arm with viable flap and external fixation still in place.
Despite the severity of the trauma, the flap demonstrated stable perfusion and progressive wound healing.
Follow-up at 6 months: Six-month follow-up showing stable coverage and acceptable contour.
The limb was preserved with stable soft-tissue coverage and improving function.

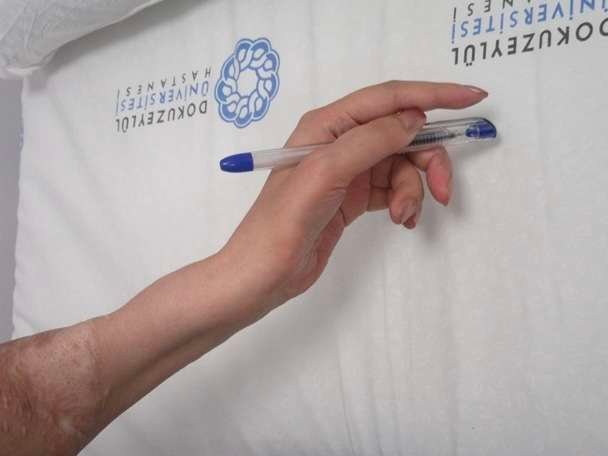
Secondary Debulking and functional refinement: To optimize contour and functional mobility, two staged debulking procedures were performed.
These images demonstrate progressive thinning of the flap and restoration of a more natural forearm contour, including the ability to hold a pen and perform fine motor tasks.

Secondary Debulking and functional refinement: To optimize contour and functional mobility, two staged debulking procedures were performed.
These images demonstrate progressive thinning of the flap and restoration of a more natural forearm contour, including the ability to hold a pen and perform fine motor tasks.

Secondary Debulking and functional refinement: To optimize contour and functional mobility, two staged debulking procedures were performed.
These images demonstrate progressive thinning of the flap and restoration of a more natural forearm contour, including the ability to hold a pen and perform fine motor tasks.
Secondary Debulking and functional refinement: To optimize contour and functional mobility, two staged debulking procedures were performed.
These images demonstrate progressive thinning of the flap and restoration of a more natural forearm contour, including the ability to hold a pen and perform fine motor tasks.
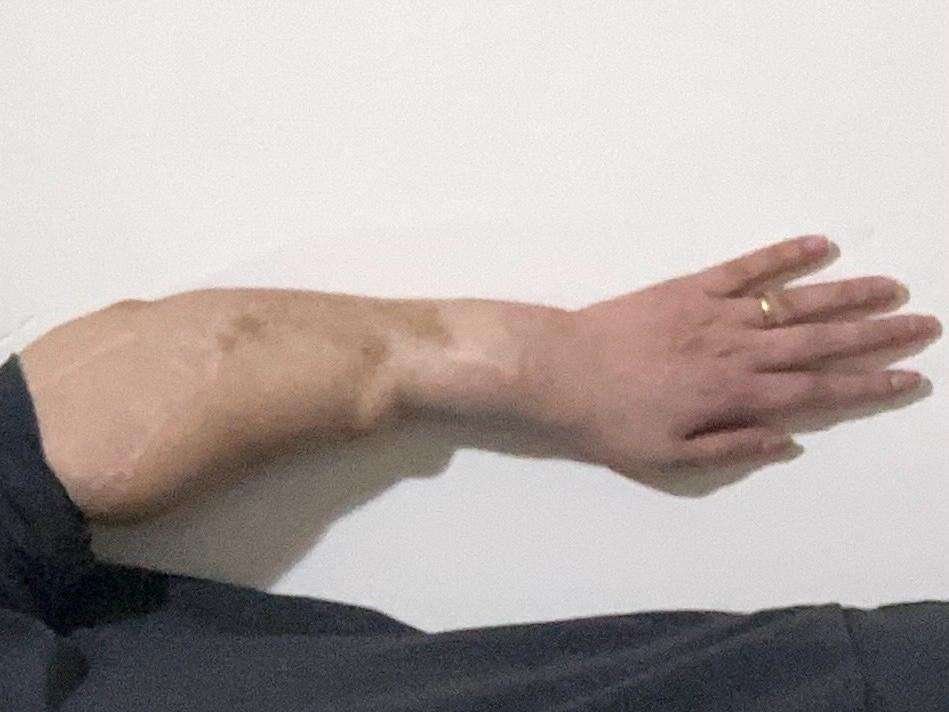
Long-term follow-up (10 years)
Ten-year postoperative photographs demonstrate durable soft-tissue coverage, stable contour, and preserved function of the salvaged upper extremity. The transferred flap has maintained a proportional relationship to the surrounding tissues and adapted harmoniously to the patient’s somatic development over time, resulting in a balanced and natural overall silhouette.
Long-term follow-up (10 years)
Ten-year postoperative photographs demonstrate durable soft-tissue coverage, stable contour, and preserved function of the salvaged upper extremity. The transferred flap has maintained a proportional relationship to the surrounding tissues and adapted harmoniously to the patient’s somatic development over time, resulting in a balanced and natural overall silhouette.

Pearls
u0026#8226; Successful limb salvage in complex trauma depends not only on surgical technique, but on close interdisciplinary coordination between trauma surgery, vascular surgery, plastic surgery, and anesthesia. In this case, standard trauma and vascular algorithms would have led to amputation, whereas a reconstructive perspective allowed a different, limb-preserving solution.
u0026#8226; Anesthetic stabilization is a critical enabler of complex emergency reconstruction. Without rapid hemodynamic control and intraoperative support, microsurgical limb salvage in critically injured patients is often not feasible [5].
u0026#8226; The combination of an anterolateral thigh flap with a vastus lateralis muscle component provides both surface coverage and deep tissue volume, which is particularly valuable in young, thin patients where an ALT flap alone may be insufficient to reconstruct extensive three-dimensional soft-tissue defects.
u0026#8226; In emergency limb-salvage situations, a pragmatic reconstructive strategy focused on the patient and on reasonable operative time is essential. Although highly sophisticated designs such as chimeric ALT–vastus lateralis flaps offer maximal intraoperative flexibility, their preparatory complexity may not be justified in critically injured patients. In our case, a myocutaneous ALT flap incorporating the vastus lateralis muscle, combined with staged secondary debulking, achieved a comparable long-term functional and contour outcome with a substantially shorter initial operative time [6-8].
u0026#8226; In young patients, a more aggressive and reconstructive-first strategy can yield a disproportionally large long-term benefit, transforming an otherwise life-long disability into a functional extremity.
Pitfalls
u0026#8226; Relying exclusively on emergency and trauma algorithms can result in amputation in cases where residual perfusion and tissue viability still permit salvage. Multidisciplinary reassessment is essential in borderline situations.
u0026#8226; Venous interposition grafts carry a substantial risk of early thrombosis and therefore require close postoperative surveillance. Graft failure should prompt immediate reassessment of limb viability rather than automatic abandonment of reconstruction.
Post-operative plan
u0026#8226; Following emergency reconstruction, the patient underwent intensive clinical flap monitoring and general condition stabilization. Early referral to hand therapy and occupational therapy was initiated to preserve joint mobility and hand function.
u0026#8226; Given the initial volume of the transferred tissues, staged secondary debulking procedures were planned and performed at appropriate intervals to refine contour, improve range of motion, and optimize the silhouette of the reconstructed forearm. Secondary contour refinement is an integral part of successful limb reconstruction, not a complication.
u0026#8226; Long-term follow-up focused on functional recovery, scar management, and progressive rehabilitation, ultimately allowing the patient to return to daily activities and professional life with preserved use of her left hand.
References
[1] Durrant CA, Mackey SP. Orthoplastic classification systems: the good, the bad, and the ungainly. Ann Plast Surg. 2011;66(1):9-12. doi:10.1097/SAP.0b013e3181f88ecf
[2] Yim GH, Hardwicke JT. The Evolution and Interpretation of the Gustilo and Anderson Classification. J Bone Joint Surg Am. 2018;100(24):e152. doi:10.2106/JBJS.18.00342
[3] Scherer J, Hax J, Teuben MPJ, Pape HC, Lefering R, Sprengel K. Epidemiology and Mortality of Surgical Amputations in Severely Injured Patients with Extremity Injuries-A Retrospective Analysis of 32,572 Patients from the TraumaRegister DGU®. J Clin Med. 2024;13(22):7000. Published 2024 Nov 20. doi:10.3390/jcm13227000
[4] Potter CBK, Bosse MJ. American Academy of Orthopaedic Surgeons Clinical Practice Guideline Summary for Limb Salvage or Early Amputation. J Am Acad Orthop Surg. 2021;29(13):e628-e634. doi:10.5435/JAAOS-D-20-00188
[5] Tobin JM, Barras WP, Bree S, et al. Anesthesia for Trauma Patients. Mil Med. 2018;183(suppl_2):32-35. doi:10.1093/milmed/usy062
[6] Wong CH, Ong YS, Wei FC. The anterolateral thigh – Vastus lateralis conjoint flap for complex defects of the lower limb. J Plast Reconstr Aesthet Surg. 2012;65(2):235-239. doi:10.1016/j.bjps.2011.08.043
[7] Lee YJ, Kim J, Lee CR, et al. Anterolateral Thigh Chimeric Flap: An Alternative Reconstructive Option to Free Flaps for Large Soft Tissue Defects. J Clin Med. 2023;12(21):6723. Published 2023 Oct 24. doi:10.3390/jcm12216723
[8] Abdelrahman M, McGarry K, Alsharkawy K, Wu JC, Cheong DC. A constant harvest technique for chimeric anterolateral thigh flaps and patient outcomes following their use in reconstructive head and neck surgery. J Plast Reconstr Aesthet Surg. 2021;74(5):1013-1021. doi:10.1016/j.bjps.2020.10.111